

Clinical course and predictive risk factors for fatal outcome of SARS-CoV-2 infection in patients with chronic kidney disease
- PMID: 33851328
- PMCID: PMC8043429
- DOI: 10.1007/s15010-021-01597-7
Clinical course and predictive risk factors for fatal outcome of SARS-CoV-2 infection in patients with chronic kidney disease
Abstract
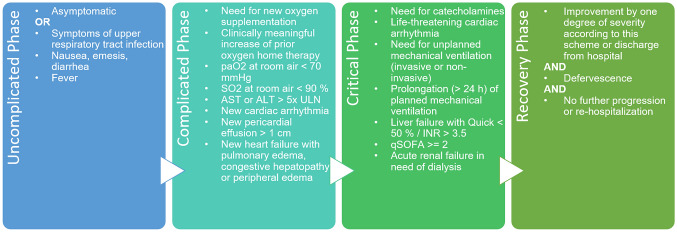
Purpose: The ongoing pandemic caused by the novel severe acute respiratory coronavirus 2 (SARS-CoV-2) has stressed health systems worldwide. Patients with chronic kidney disease (CKD) seem to be more prone to a severe course of coronavirus disease (COVID-19) due to comorbidities and an altered immune system. The study's aim was to identify factors predicting mortality among SARS-CoV-2-infected patients with CKD.
Methods: We analyzed 2817 SARS-CoV-2-infected patients enrolled in the Lean European Open Survey on SARS-CoV-2-infected patients and identified 426 patients with pre-existing CKD. Group comparisons were performed via Chi-squared test. Using univariate and multivariable logistic regression, predictive factors for mortality were identified.
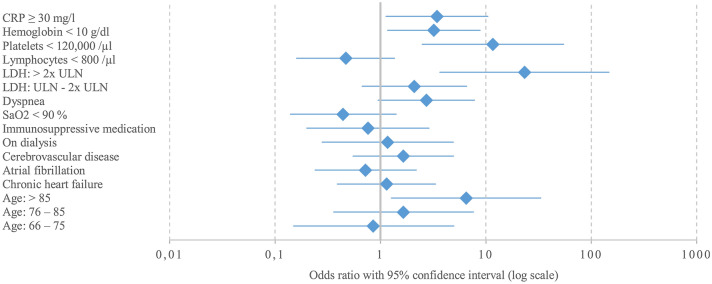
Results: Comparative analyses to patients without CKD revealed a higher mortality (140/426, 32.9% versus 354/2391, 14.8%). Higher age could be confirmed as a demographic predictor for mortality in CKD patients (> 85 years compared to 15-65 years, adjusted odds ratio (aOR) 6.49, 95% CI 1.27-33.20, p = 0.025). We further identified markedly elevated lactate dehydrogenase (> 2 × upper limit of normal, aOR 23.21, 95% CI 3.66-147.11, p < 0.001), thrombocytopenia (< 120,000/µl, aOR 11.66, 95% CI 2.49-54.70, p = 0.002), anemia (Hb < 10 g/dl, aOR 3.21, 95% CI 1.17-8.82, p = 0.024), and C-reactive protein (≥ 30 mg/l, aOR 3.44, 95% CI 1.13-10.45, p = 0.029) as predictors, while renal replacement therapy was not related to mortality (aOR 1.15, 95% CI 0.68-1.93, p = 0.611).
Conclusion: The identified predictors include routinely measured and universally available parameters. Their assessment might facilitate risk stratification in this highly vulnerable cohort as early as at initial medical evaluation for SARS-CoV-2.
Keywords: COVID-19; Chronic kidney disease; LEOSS; Predictive factor; SARS-CoV-2.
© 2021. The Author(s).
Conflict of interest statement
Felix C. Koehler is supported by the Koeln Fortune program/Faculty of Medicine, University of Cologne, and has received grants from the Maria-Pesch Stiftung, Cologne, Germany and from the German Federal Ministry of Research and Education, and non-financial support from Miltenyi Biotec GmbH, Bergisch Gladbach, Germany outside the submitted work. Lisa Pilgram received a grant from DZIF (German Center for Infection Research) and Willy Robert Pitzer Foundation. All authors declare no relevant conflicts of interest.
Figures
References
-
- Ding Y, He L, Zhang Q, Huang Z, Che X, Hou J, et al. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: implications for pathogenesis and virus transmission pathways. J Pathol. 2004;203:622–630. doi: 10.1002/path.1560. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
