

Single Nucleotide Polymorphisms (SNPs) in PRKG1 & SPATA13-AS1 are associated with bronchodilator response: a pilot study during acute asthma exacerbations in African American children
- PMID: 33851947
- PMCID: PMC8373649
- DOI: 10.1097/FPC.0000000000000434
Single Nucleotide Polymorphisms (SNPs) in PRKG1 & SPATA13-AS1 are associated with bronchodilator response: a pilot study during acute asthma exacerbations in African American children
Abstract
Objective: Inhaled bronchodilators are the first-line treatment for asthma exacerbations, but individual bronchodilator response (BDR) varies by race and ethnicity. Studies have examined BDR's genetic underpinnings, but many did not include children or were not conducted during an asthma exacerbation. This pilot study tested single-nucleotide polymorphisms' (SNPs') association with pediatric African American BDR during an acute asthma exacerbation.
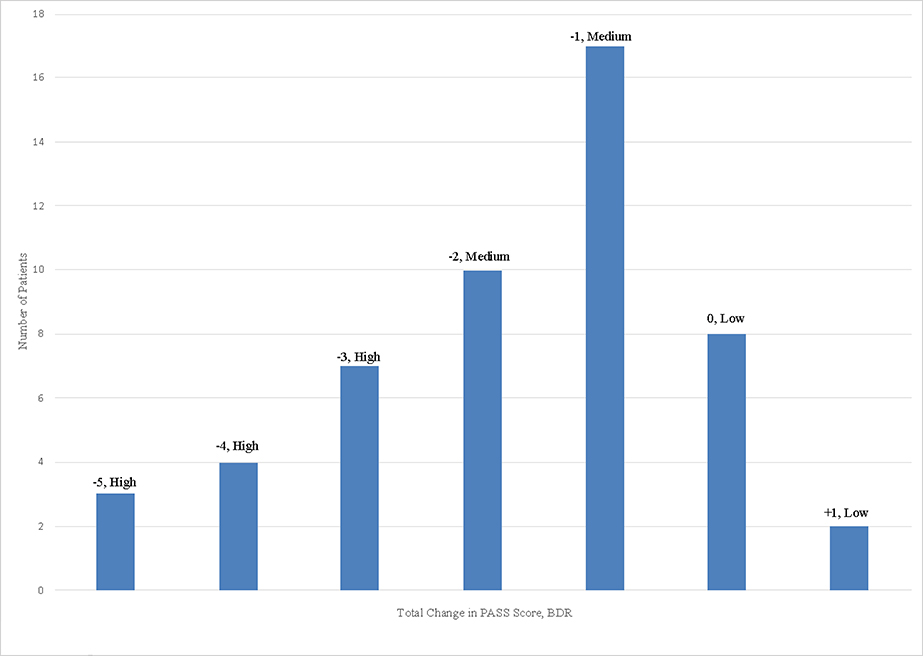
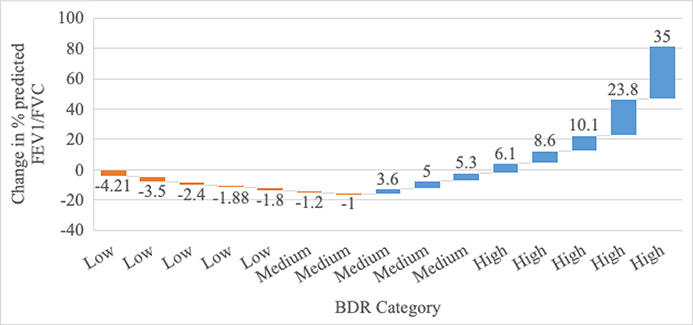
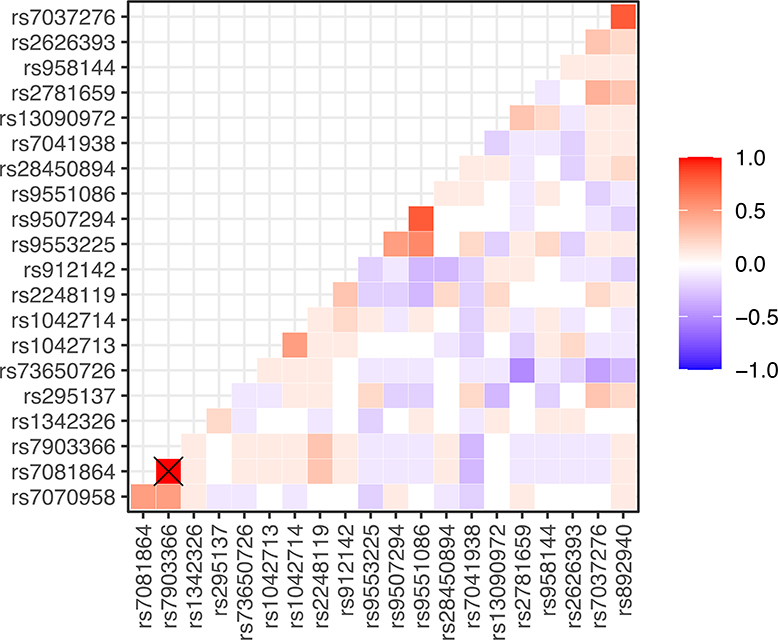
Methods: This was a study of pediatric asthma patients in the age group 2-18 years treated in the emergency department for an asthma exacerbation. We measured BDR before and after inhaled bronchodilator treatments using both the Pediatric Asthma Severity Score (PASS) and asthma severity score. We collected genomic DNA and examined whether 21 candidate SNPs from a review of the literature were associated with BDR using crude odds ratios (OR) and adjusted analysis.
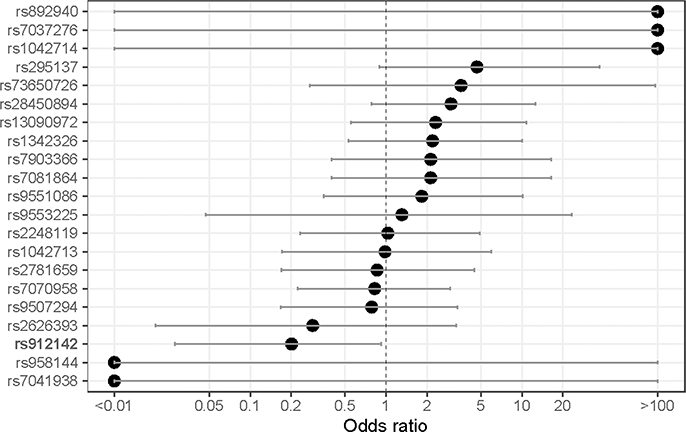
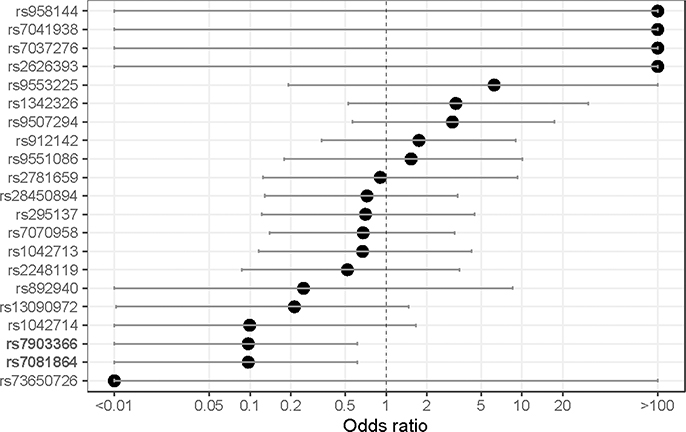
Results: The final sample population was 53 children, with an average age of 7.2 years. The average initial PASS score (scale of ascending severity from 0 to 6) was 2.5. After adjusting for BMI, age category, gender and smoke exposure, rs912142 was associated with decreased odds of having low BDR (OR, 0.20; 95% confidence interval (CI), 0.02-0.92), and rs7081864 and rs7903366 were associated with decreased odds of having high BDR (OR, 0.097; 95% CI, 0.009-0.62).
Conclusions: We found three SNPs significantly associated with pediatric African American BDR that provide information regarding a child's potential response to emergency asthma exacerbation treatment. Once validated in larger studies, such information could guide pharmacogenomic evidence-based emergency asthma treatment to improve patient outcomes.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Asthma Facts: CDC’s National Asthma Control Program Grantees. 2013Available at https://www.cdc.gov/asthma/pdfs/asthma_facts_program_grantees.pdf.Accessed September 26, 2018.
-
- Centers for Disease Control and Prevention. 2015 National Health Interview Survey Data. Available at: https://www.cdc.gov/asthma/most_recent_data.htm.Accessed September 26, 2018.
-
- Mannino DM, Homa DM, Akinbami LJ, Moorman JE, Gwynn C, Redd SC. Surveillance for asthma—United States, 1980–1999. MMWR Surveill Summ. 2002;51(1):1–13. - PubMed
-
- Newacheck PW, Halfon N. Prevalence, impact, and trends in childhood disability due to asthma. Arch Pediatr Adolesc Med. 2000;154(3):287–93. - PubMed
-
- Akinbami LJ, Moorman JE, Liu X. Asthma prevalence, health care use, and mortality: United States, 2005–2009. Natl Health Stat Report. 2011;12(32):1–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
