

Association of Intravenous Tranexamic Acid With Thromboembolic Events and Mortality: A Systematic Review, Meta-analysis, and Meta-regression
- PMID: 33851983
- PMCID: PMC8047805
- DOI: 10.1001/jamasurg.2021.0884
Association of Intravenous Tranexamic Acid With Thromboembolic Events and Mortality: A Systematic Review, Meta-analysis, and Meta-regression
Abstract
Importance: Tranexamic acid (TXA) is an efficient antifibrinolytic agent; however, concerns remain about the potential adverse effects, particularly vascular occlusive events, that may be associated with its use.
Objective: To examine the association between intravenous TXA and total thromboembolic events (TEs) and mortality in patients of all ages and of any medical disciplines.
Data source: Cochrane Central Register of Controlled Trials and MEDLINE were searched for eligible studies investigating intravenous TXA and postinterventional outcome published between 1976 and 2020.
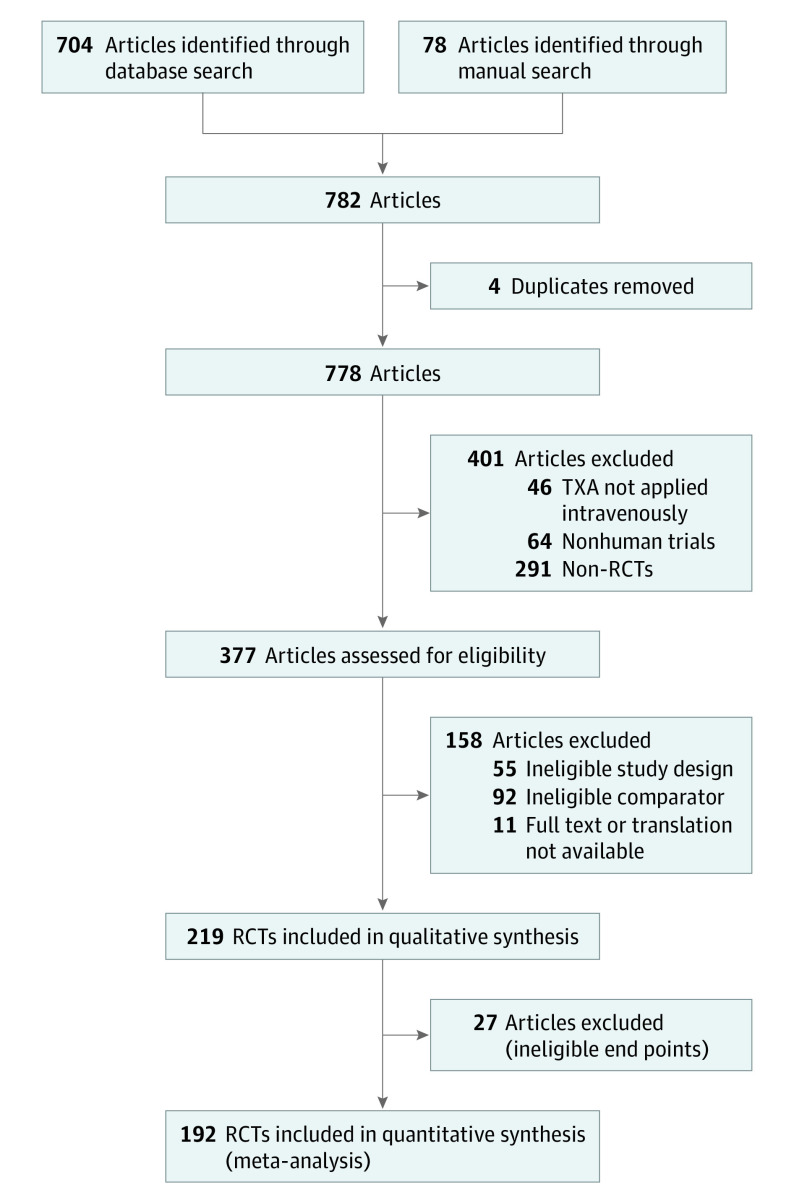
Study selection: Randomized clinical trials comparing intravenous TXA with placebo/no treatment. The electronic database search yielded a total of 782 studies, and 381 were considered for full-text review. Included studies were published in English, German, French, and Spanish. Studies with only oral or topical tranexamic administration were excluded.
Data extraction and synthesis: Meta-analysis, subgroup and sensitivity analysis, and meta-regression were performed. This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Main outcomes and measures: Vascular occlusive events and mortality.
Results: A total of 216 eligible trials including 125 550 patients were analyzed. Total TEs were found in 1020 (2.1%) in the group receiving TXA and 900 (2.0%) in the control group. This study found no association between TXA and risk for total TEs (risk difference = 0.001; 95% CI, -0.001 to 0.002; P = .49) for venous thrombosis, pulmonary embolism, venous TEs, myocardial infarction or ischemia, and cerebral infarction or ischemia. Sensitivity analysis using the risk ratio as an effect measure with (risk ratio = 1.02; 95% CI, 0.94-1.11; P = .56) and without (risk ratio = 1.03; 95% CI, 0.95-1.12; P = .52) studies with double-zero events revealed robust effect size estimates. Sensitivity analysis with studies judged at low risk for selection bias showed similar results. Administration of TXA was associated with a significant reduction in overall mortality and bleeding mortality but not with nonbleeding mortality. In addition, an increased risk for vascular occlusive events was not found in studies including patients with a history of thromboembolism. Comparison of studies with sample sizes of less than or equal to 99 (risk difference = 0.004; 95% CI, -0.006 to 0.014; P = .40), 100 to 999 (risk difference = 0.004; 95% CI, -0.003 to 0.011; P = .26), and greater than or equal to 1000 (risk difference = -0.001; 95% CI, -0.003 to 0.001; P = .44) showed no association between TXA and incidence of total TEs. Meta-regression of 143 intervention groups showed no association between TXA dosing and risk for venous TEs (risk difference, -0.005; 95% CI, -0.021 to 0.011; P = .53).
Conclusions and relevance: Findings from this systematic review and meta-analysis of 216 studies suggested that intravenous TXA, irrespective of dosing, is not associated with increased risk of any TE. These results help clarify the incidence of adverse events associated with administration of intravenous TXA and suggest that TXA is safe for use with undetermined utility for patients receiving neurological care.
Conflict of interest statement
Figures
Comment in
-
Importance of the Assessment Time Window for Intravenous Tranexamic Acid and Thromboembolic Events.JAMA Surg. 2022 Jan 1;157(1):79-80. doi: 10.1001/jamasurg.2021.4138. JAMA Surg. 2022. PMID: 34468702 No abstract available.
-
Importance of the Assessment Time Window for Intravenous Tranexamic Acid and Thromboembolic Events-Reply.JAMA Surg. 2022 Jan 1;157(1):80-81. doi: 10.1001/jamasurg.2021.4141. JAMA Surg. 2022. PMID: 34468712 No abstract available.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
