

Perioperative hemodynamic optimization: from guidelines to implementation-an experts' opinion paper
- PMID: 33852124
- PMCID: PMC8046882
- DOI: 10.1186/s13613-021-00845-1
Perioperative hemodynamic optimization: from guidelines to implementation-an experts' opinion paper
Abstract
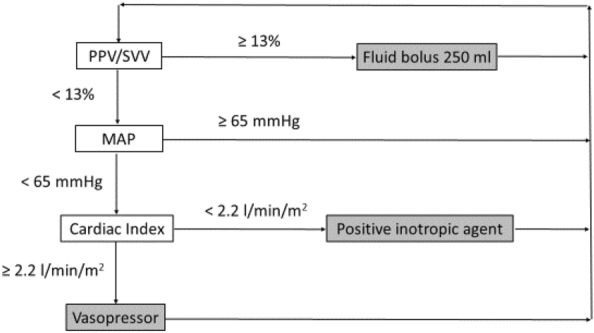
Despite a large body of evidence, the implementation of guidelines on hemodynamic optimization and goal-directed therapy remains limited in daily routine practice. To facilitate/accelerate this implementation, a panel of experts in the field proposes an approach based on six relevant questions/answers that are frequently mentioned by clinicians, using a critical appraisal of the literature and a modified Delphi process. The mean arterial pressure is a major determinant of organ perfusion, so that the authors unanimously recommend not to tolerate absolute values below 65 mmHg during surgery to reduce the risk of postoperative organ dysfunction. Despite well-identified limitations, the authors unanimously propose the use of dynamic indices to rationalize fluid therapy in a large number of patients undergoing non-cardiac surgery, pending the implementation of a "validity criteria checklist" before applying volume expansion. The authors recommend with a good agreement mini- or non-invasive stroke volume/cardiac output monitoring in moderate to high-risk surgical patients to optimize fluid therapy on an individual basis and avoid volume overload. The authors propose to use fluids and vasoconstrictors in combination to achieve optimal blood flow and maintain perfusion pressure above the thresholds considered at risk. Although purchase of disposable sensors and stand-alone monitors will result in additional costs, the authors unanimously acknowledge that there are data strongly suggesting this may be counterbalanced by a sustained reduction in postoperative morbidity and hospital lengths of stay. Beside existing guidelines, knowledge and explicit clinical reasoning tools followed by decision algorithms are mandatory to implement individualized hemodynamic optimization strategies and reduce postoperative morbidity and duration of hospital stay in high-risk surgical patients.
Keywords: Blood pressure; Fluid responsiveness; Health costs; Hemodynamic optimization; High-risk surgery; Perioperative morbidity; Vasopressors.
Conflict of interest statement
JLF, EF, CV, OC, OH, JL, KA, BC, and DL are members of an advisory board working for Edwards Lifesciences and have received honoraria from the Company for their participation to the board. JLF and DL have received honoraria from Masimo for participation to hemodynamic master classes. EF reported receiving consulting fees from Drager Medical, GE Healthcare, and Orion Pharma and lecture fees from Fresenius Kabi, Baxter, and Fisher and Paykel Healthcare. EG has received lecture fees from Edwards Lifesciences and research support from Philips and Radiometer. MB has received lecture fees from Edwards Lifesciences and Maquet Pulsion. KA has received lecture fees from LFB, Fisher and Paykel Healthcare, and Baxter. BT has no conflicts of interest to declare.
Figures
References
-
- Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, et al. European Surgical Outcomes Study (EuSOS) group for the Trials groups of the European Society of Intensive Care Medicine and the European Society of Anaesthesiology. Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012;380:1059–65. doi: 10.1016/S0140-6736(12)61148-9. - DOI - PMC - PubMed
-
- Som A, Maitra S, Bhattacharjee S, Baidya DK. Goal directed fluid therapy decreases postoperative morbidity but not mortality in major non-cardiac surgery: a meta-analysis and trial sequential analysis of randomized controlled trials. J Anesth. 2017;31:66–81. doi: 10.1007/s00540-016-2261-7. - DOI - PubMed
-
- Messina A, Robba C, Calabro L, Zambelli D, Lannuzzi F, Molinari E, et al. Association between perioperative fluid administration and postoperative outcomes: a 20-year systematic review and a meta-analysis of randomized goal-directed trials in major visceral/noncardiac surgery. Crit Care. 2021;25:43. doi: 10.1186/s13054-021-03464-1. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
