

Short-term morbidity and mortality following radical cystectomy: a systematic review
- PMID: 33853799
- PMCID: PMC8054090
- DOI: 10.1136/bmjopen-2020-043266
Short-term morbidity and mortality following radical cystectomy: a systematic review
Abstract
Objective: To study short-term (<90 days) morbidity and mortality following radical cystectomy (RC) for bladder cancer and identify modifiable risk factors associated with these.
Design: Systematic review.
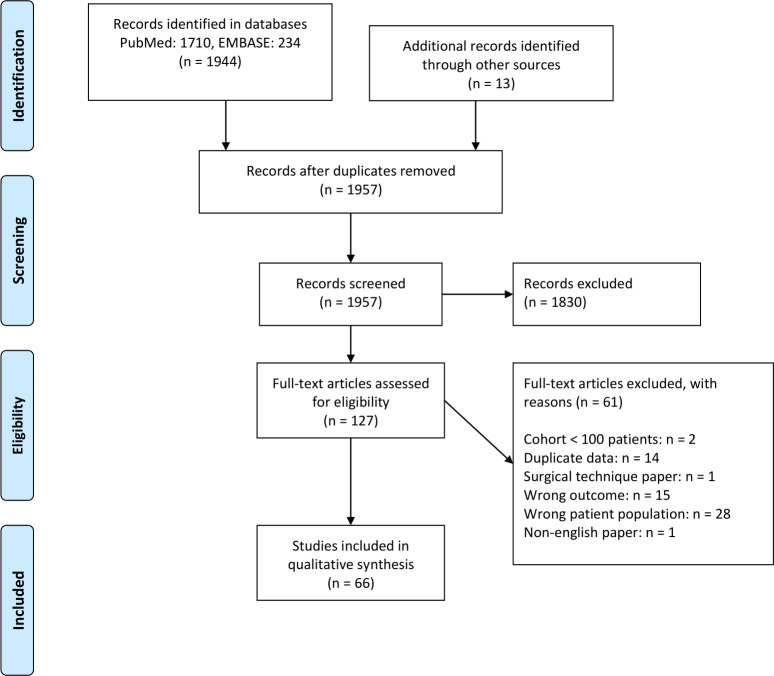
Methods: The systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. PubMed and EMBASE were searched for relevant papers on 11 June 2019 and rerun on 27 May 2020. Studies reporting complications, reoperations, length of stay and mortality within 90 days were included. Studies were reviewed according to criteria from the Oxford Centre for Evidence-Based Medicine and the quality of evidence was assessed using the Newcastle-Ottawa Scale.
Results: The search retrieved 1957 articles. Sixty-six articles were included. The quality of evidence was poor to good. Most studies were retrospective, and no randomised clinical trials were identified. Of included studies a median of 6 Martin criteria for reporting complications after surgery were fulfilled. The Clavien-Dindo classification for grading complications was most frequently used. The weighted overall complication rate after RC was 34.9% (range 28.8-68.8) for in-house complications, 39.0% (range 27.3-80.0) for 30-day complications and 58.5% (range 36.1-80.5) for 90-day complications. The most common types of complications reported were gastrointestinal (29.0%) and infectious (26.4%). The weighted mortality rate was 2.4% (range 0.9-4.7) for in-house mortality, 2.1% (0.0-3.7) for 30-day mortality and 4.7% (range 0.0-7.0) for 90-day mortality. Age and comorbidity were identified as the best predictors for complications following RC.
Conclusion: Short-term morbidity and mortality are high following RC. Reporting of complications is heterogeneous and the quality of evidence is generally low. There is a continuous need for randomised studies to address any intervention that can reduce morbidity and mortality following RC.
Prospero registration number: 104937.
Keywords: bladder disorders; surgery; urological tumours.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Covidence . Covidence systematic review software [Internet]. Veritas Health Innovation Ltd, Melbourne, Australia. Available: www.covidence.org
-
- Howick J, Chalmers I, Glasziou P. The Oxford 2011 levels of evidence”. Oxford centre for evidence-based medicine. [Internet]. Available: http://www.cebm.net/index.aspx?o=5653
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical