

Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies
- PMID: 33853828
- PMCID: PMC8044922
- DOI: 10.1136/bmj.n604
Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies
Abstract
Objective: To examine whether overall lifestyles mediate associations of socioeconomic status (SES) with mortality and incident cardiovascular disease (CVD) and the extent of interaction or joint relations of lifestyles and SES with health outcomes.
Design: Population based cohort study.
Setting: US National Health and Nutrition Examination Survey (US NHANES, 1988-94 and 1999-2014) and UK Biobank.
Participants: 44 462 US adults aged 20 years or older and 399 537 UK adults aged 37-73 years.
Exposures: SES was derived by latent class analysis using family income, occupation or employment status, education level, and health insurance (US NHANES only), and three levels (low, medium, and high) were defined according to item response probabilities. A healthy lifestyle score was constructed using information on never smoking, no heavy alcohol consumption (women ≤1 drink/day; men ≤2 drinks/day; one drink contains 14 g of ethanol in the US and 8 g in the UK), top third of physical activity, and higher dietary quality.
Main outcome measures: All cause mortality was the primary outcome in both studies, and CVD mortality and morbidity in UK Biobank, which were obtained through linkage to registries.
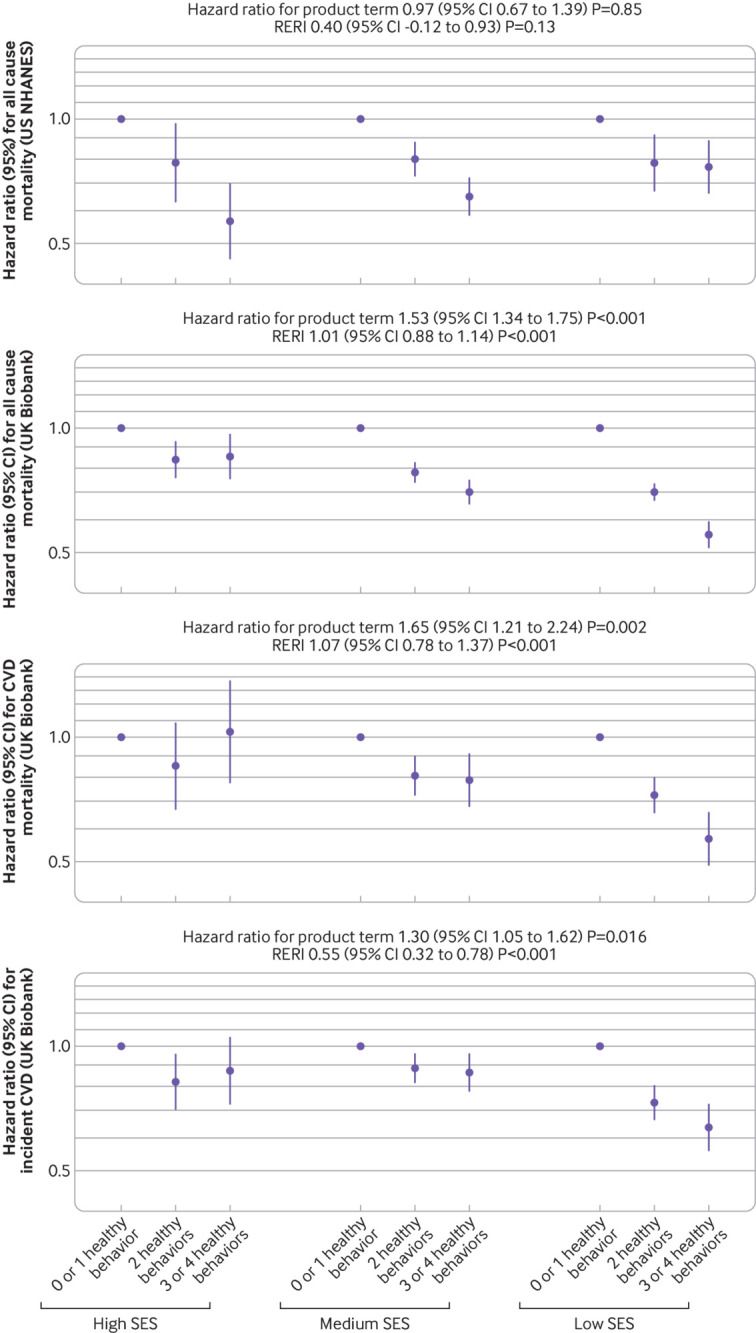
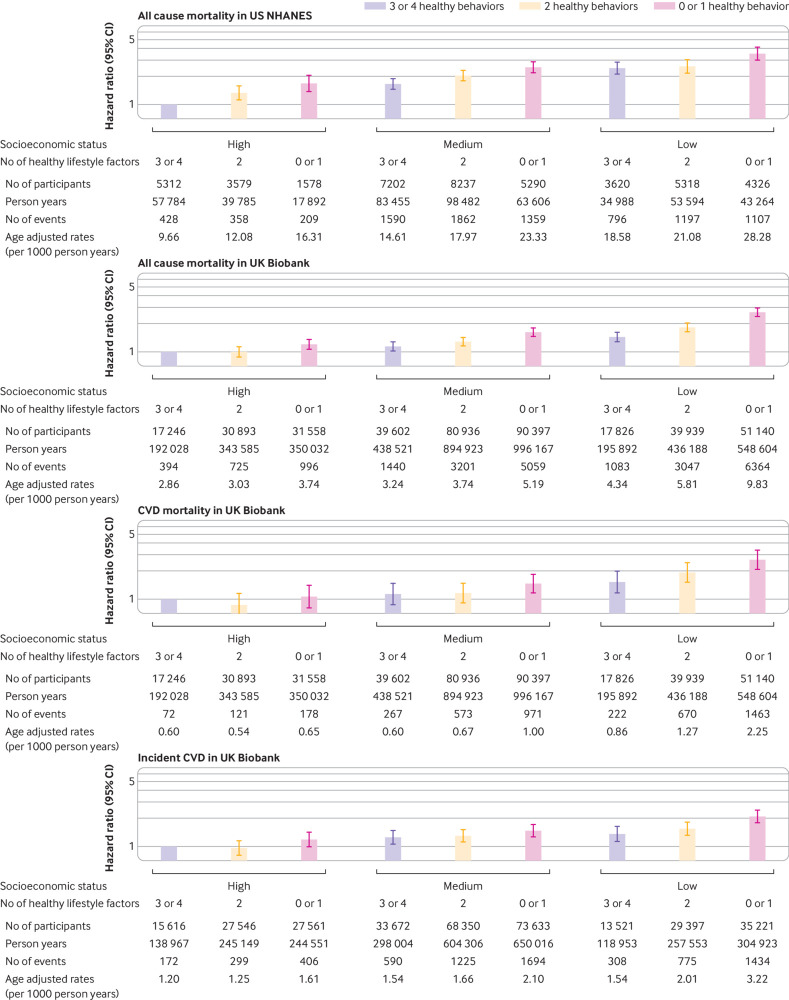
Results: US NHANES documented 8906 deaths over a mean follow-up of 11.2 years, and UK Biobank documented 22 309 deaths and 6903 incident CVD cases over a mean follow-up of 8.8-11.0 years. Among adults of low SES, age adjusted risk of death was 22.5 (95% confidence interval 21.7 to 23.3) and 7.4 (7.3 to 7.6) per 1000 person years in US NHANES and UK Biobank, respectively, and age adjusted risk of CVD was 2.5 (2.4 to 2.6) per 1000 person years in UK Biobank. The corresponding risks among adults of high SES were 11.4 (10.6 to 12.1), 3.3 (3.1 to 3.5), and 1.4 (1.3 to 1.5) per 1000 person years. Compared with adults of high SES, those of low SES had higher risks of all cause mortality (hazard ratio 2.13, 95% confidence interval 1.90 to 2.38 in US NHANES; 1.96, 1.87 to 2.06 in UK Biobank), CVD mortality (2.25, 2.00 to 2.53), and incident CVD (1.65, 1.52 to 1.79) in UK Biobank, and the proportions mediated by lifestyle were 12.3% (10.7% to 13.9%), 4.0% (3.5% to 4.4%), 3.0% (2.5% to 3.6%), and 3.7% (3.1% to 4.5%), respectively. No significant interaction was observed between lifestyle and SES in US NHANES, whereas associations between lifestyle and outcomes were stronger among those of low SES in UK Biobank. Compared with adults of high SES and three or four healthy lifestyle factors, those with low SES and no or one healthy lifestyle factor had higher risks of all cause mortality (3.53, 3.01 to 4.14 in US NHANES; 2.65, 2.39 to 2.94 in UK Biobank), CVD mortality (2.65, 2.09 to 3.38), and incident CVD (2.09, 1.78 to 2.46) in UK Biobank.
Conclusions: Unhealthy lifestyles mediated a small proportion of the socioeconomic inequity in health in both US and UK adults; therefore, healthy lifestyle promotion alone might not substantially reduce the socioeconomic inequity in health, and other measures tackling social determinants of health are warranted. Nevertheless, healthy lifestyles were associated with lower mortality and CVD risk in different SES subgroups, supporting an important role of healthy lifestyles in reducing disease burden.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Nature Science Foundation of China and National Key Research and Development Program of China (AP) for the submitted work; support from California Walnut Committee and Swiss Reinsurance Company (YL) outside the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Public health needs to go back to basics, not rely on nudge theory.BMJ. 2021 May 6;373:n1153. doi: 10.1136/bmj.n1153. BMJ. 2021. PMID: 33958378 No abstract available.
-
Gesunde Ernährung allein reicht oft nicht.MMW Fortschr Med. 2023 Feb;165(3):73. doi: 10.1007/s15006-023-2359-4. MMW Fortschr Med. 2023. PMID: 36759485 German. No abstract available.
References
-
- Marmot M, Allen J, Boyce T, Goldblatt P, Morrison M. Health equity in England: the Marmot review ten years on. 2020. www.health.org.uk/publications/reports/the-marmot-review-10-years-on.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical