

Imaging Enterobacterales infections in patients using pathogen-specific positron emission tomography
- PMID: 33853931
- PMCID: PMC8120649
- DOI: 10.1126/scitranslmed.abe9805
Imaging Enterobacterales infections in patients using pathogen-specific positron emission tomography
Abstract
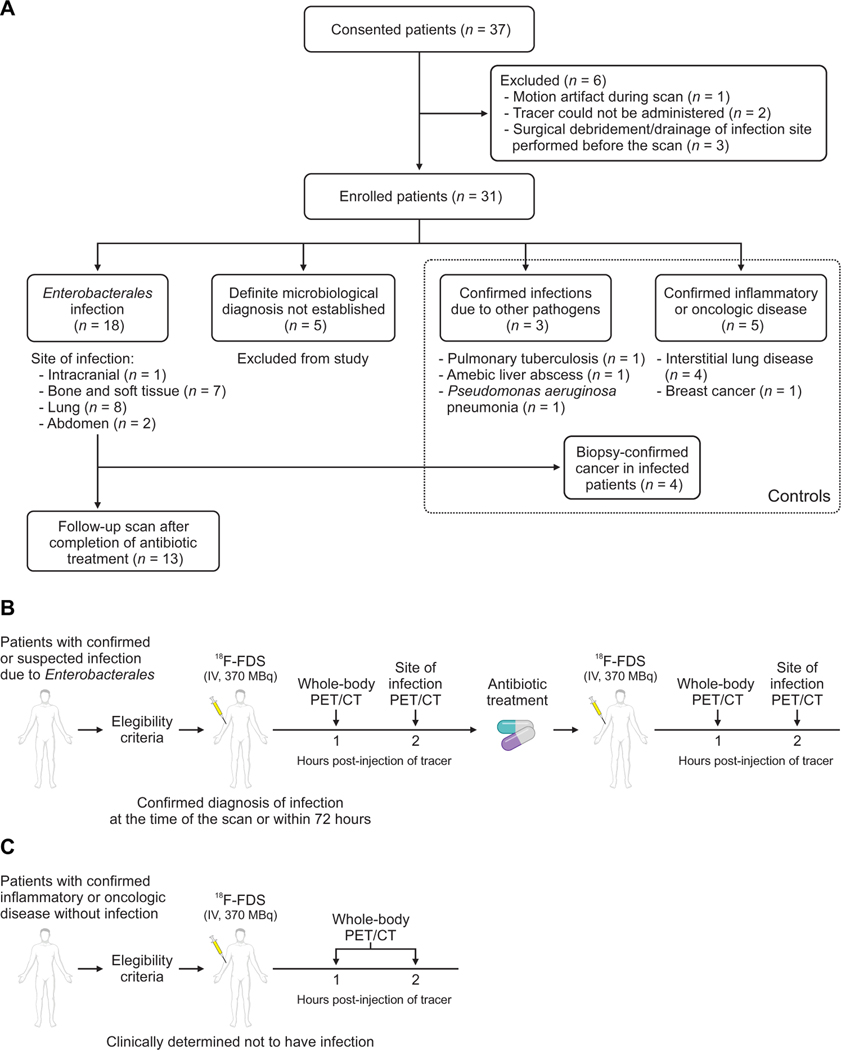
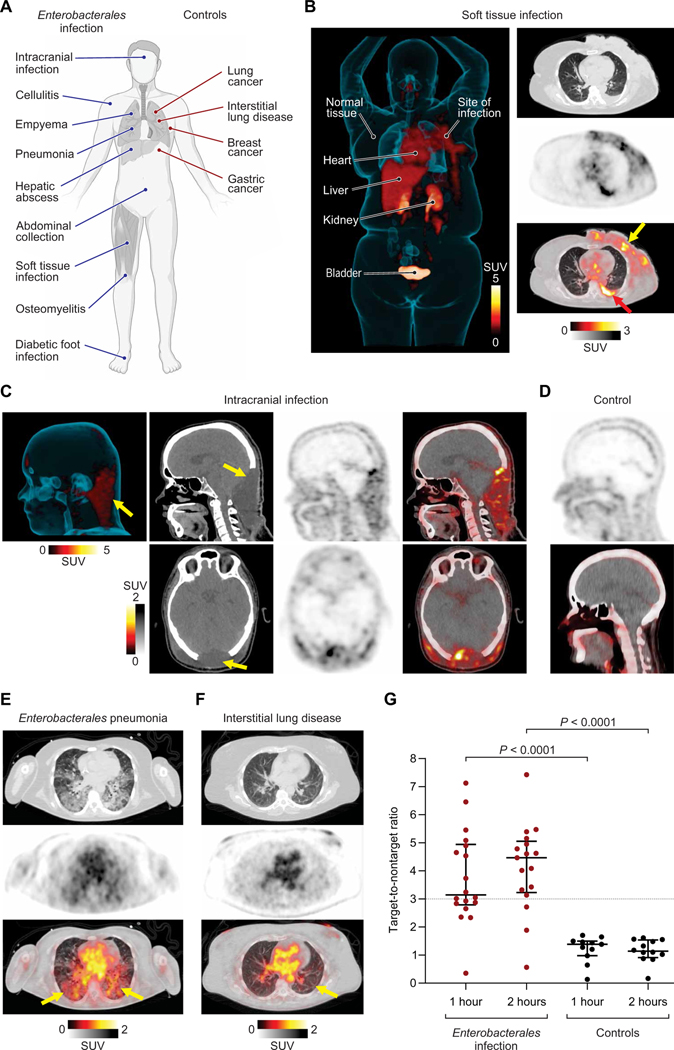
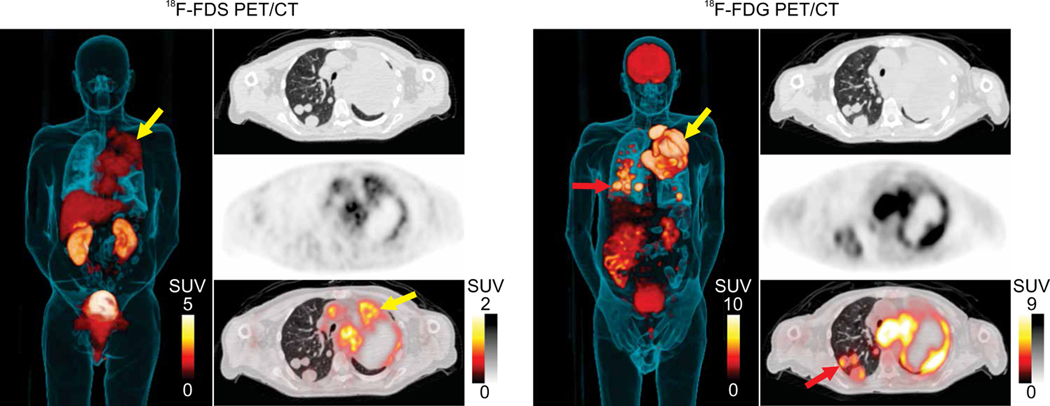
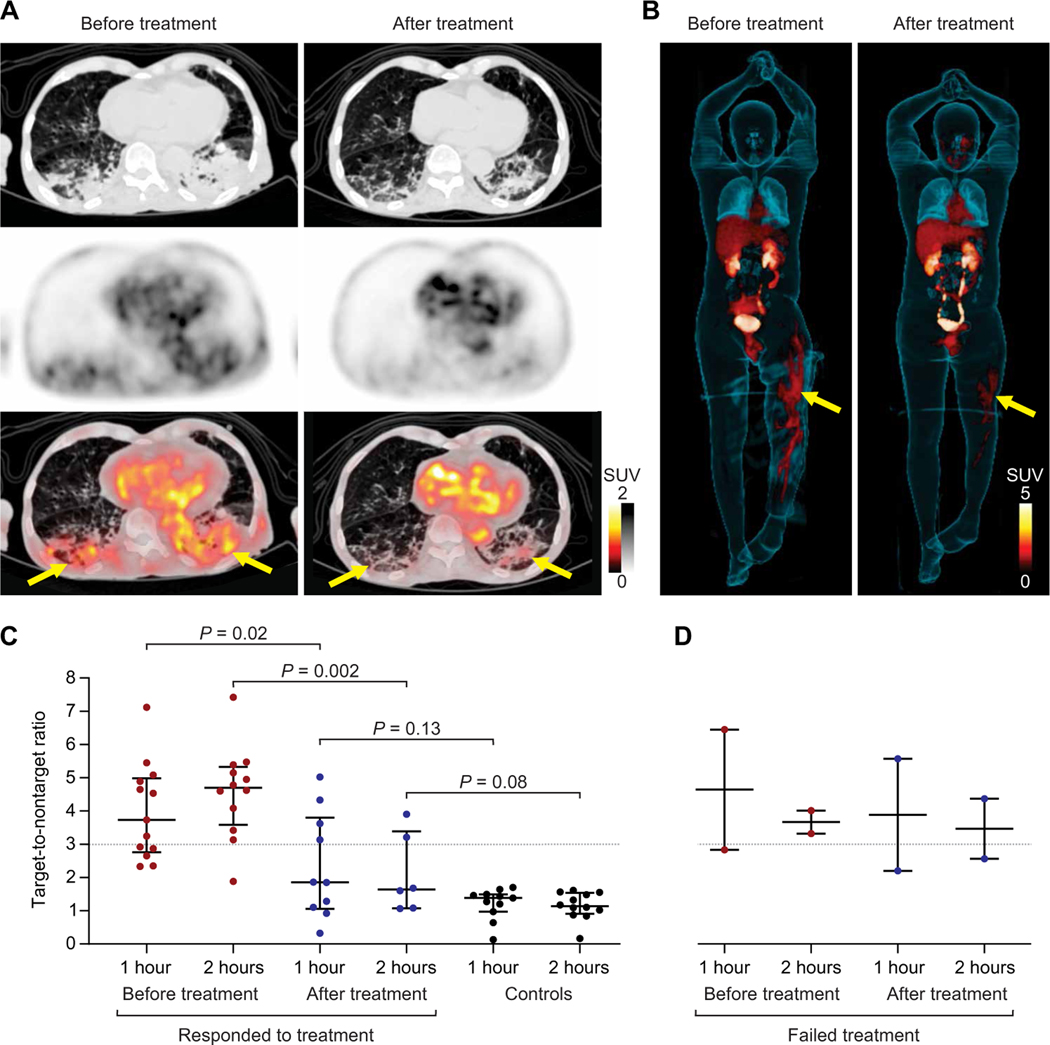
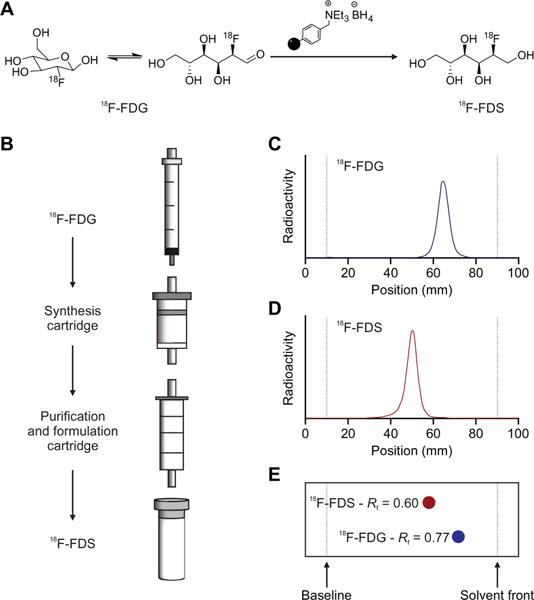
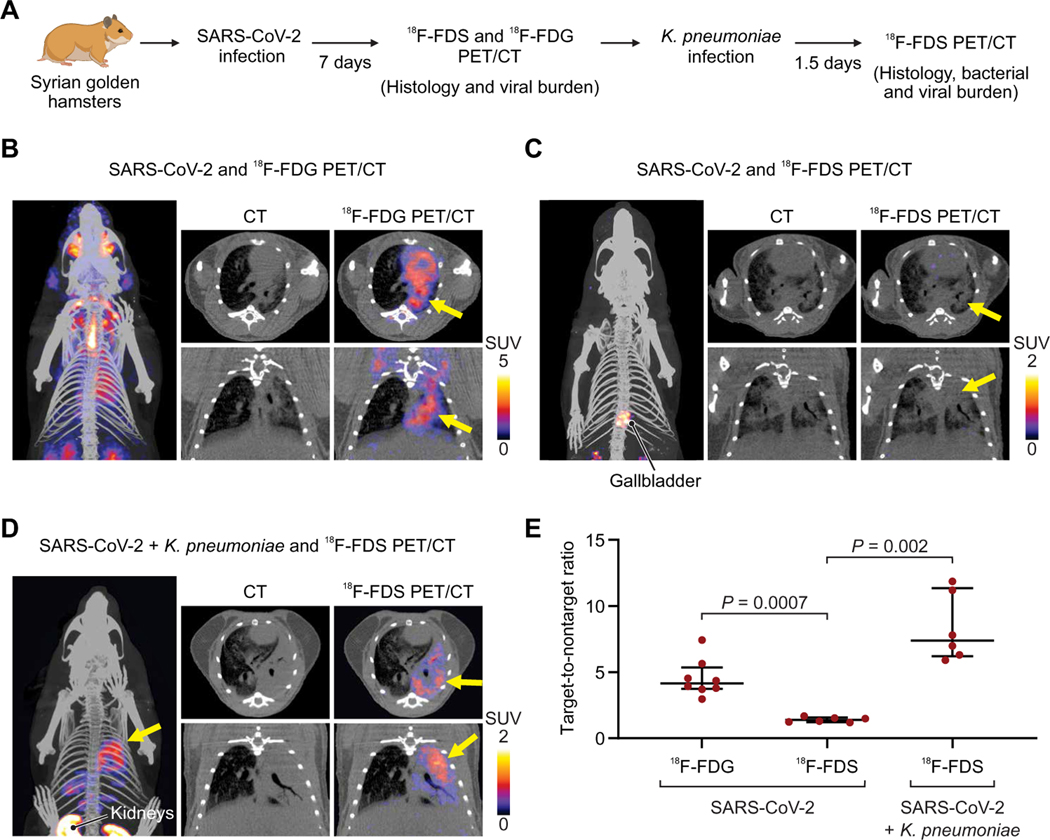
Enterobacterales represent the largest group of bacterial pathogens in humans and are responsible for severe, deep-seated infections, often resulting in sepsis or death. They are also a prominent cause of multidrug-resistant (MDR) infections, and some species are recognized as biothreat pathogens. Tools for noninvasive, whole-body analysis that can localize a pathogen with specificity are needed, but no such technology currently exists. We previously demonstrated that positron emission tomography (PET) with 2-deoxy-2-[18F]fluoro-d-sorbitol (18F-FDS) can selectively detect Enterobacterales infections in murine models. Here, we demonstrate that uptake of 18F-FDS by bacteria occurs via a metabolically conserved sorbitol-specific pathway with rapid in vitro 18F-FDS uptake noted in clinical strains, including MDR isolates. Whole-body 18F-FDS PET/computerized tomography (CT) in 26 prospectively enrolled patients with either microbiologically confirmed Enterobacterales infection or other pathologies demonstrated that 18F-FDS PET/CT was safe, could rapidly detect and localize Enterobacterales infections due to drug-susceptible or MDR strains, and differentiated them from sterile inflammation or cancerous lesions. Repeat imaging in the same patients monitored antibiotic efficacy with decreases in PET signal correlating with clinical improvement. To facilitate the use of 18F-FDS, we developed a self-contained, solid-phase cartridge to rapidly (<10 min) formulate ready-to-use 18F-FDS from commercially available 2-deoxy-2-[18F]fluoro-d-glucose (18F-FDG) at room temperature. In a hamster model, 18F-FDS PET/CT also differentiated severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia from secondary Klebsiella pneumoniae pneumonia-a leading cause of complications in hospitalized patients with COVID-19. These data support 18F-FDS as an innovative and readily available, pathogen-specific PET technology with clinical applications.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
References
-
- Donnenberg MS, Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, Gerald JEB Mandell L, Dolin R, Eds. (Elsevier Inc., 2010), chap. 218, pp. 2815–2833.
-
- Guentzel MN, in Medical Microbiology, Baron S, Ed. (University of Texas Medical Branch at Galveston, 1996), chap. 26. - PubMed
-
- Centers for Disease Control and Prevention, Antibiotic Resistance Threats in the United States (Centers for Disease Control and Prevention, 2019); https://cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report....
-
- Dhesi Z, Enne VI, Brealey D, Livermore DM, High J, Russell C, Colles A, Kandil H, Mack D, Martin D, Page V, Parker R, Roulston K, Singh S, Wey E, Swart AM, Stirling S, Barber JA, O’Grady J, Gant VA, Organisms causing secondary pneumonias in COVID-19 patients at 5 UK ICUs as detected with the FilmArray test. medRxiv 10.1101/2020.2006.2022.20131573, (2020). - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
