

Genetic basis of hypercholesterolemia in adults
- PMID: 33854068
- PMCID: PMC8046820
- DOI: 10.1038/s41525-021-00190-z
Genetic basis of hypercholesterolemia in adults
Erratum in
-
Author Correction: Genetic basis of hypercholesterolemia in adults.NPJ Genom Med. 2021 Jun 29;6(1):56. doi: 10.1038/s41525-021-00222-8. NPJ Genom Med. 2021. PMID: 34188061 Free PMC article. No abstract available.
Abstract
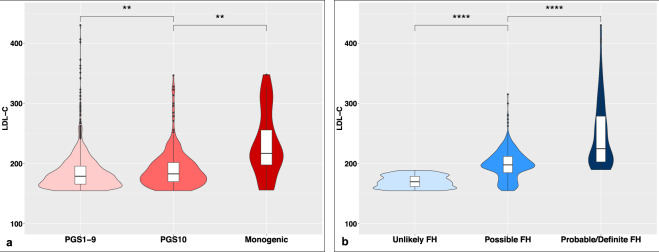
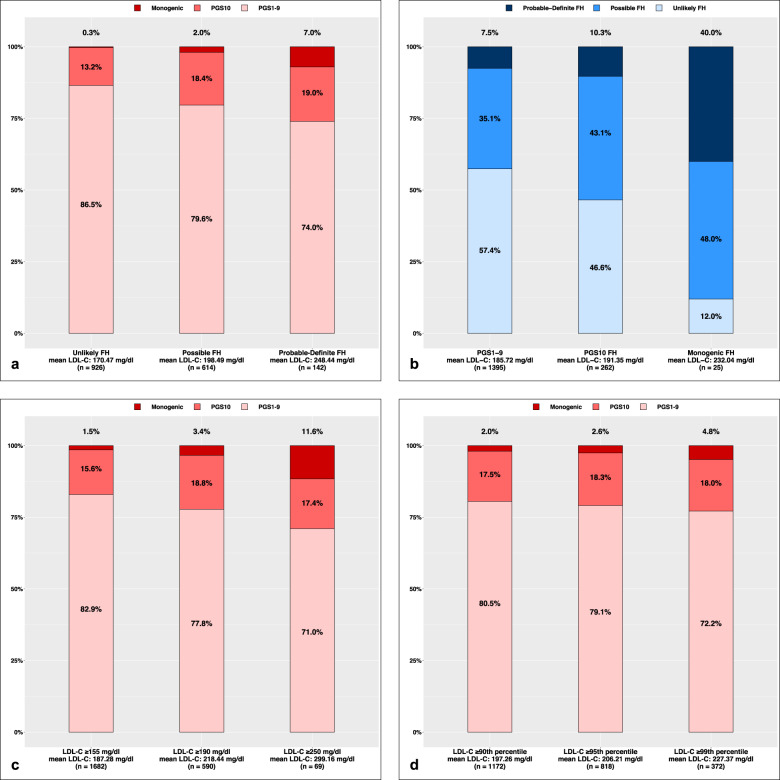
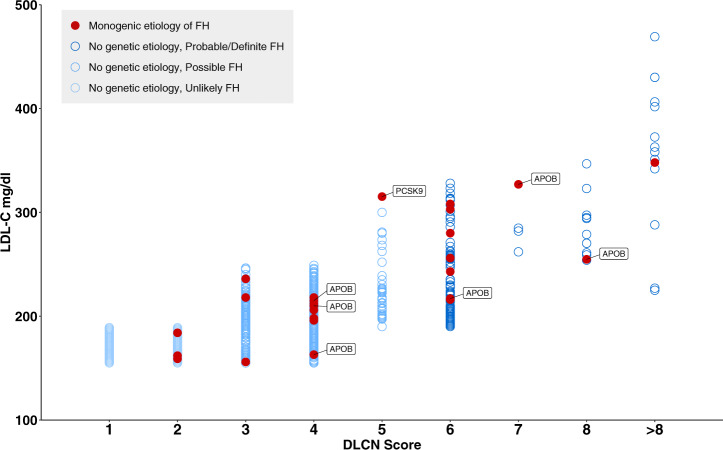
We investigated monogenic and polygenic causes of hypercholesterolemia in a population-based cohort, excluding secondary hypercholesterolemia, and using an established framework to identify pathogenic variants. We studied 1682 individuals (50.2 ± 8.6 years, 41.3% males) from southeast Minnesota with primary hypercholesterolemia (low-density lipoprotein cholesterol (LDL-C) ≥155 mg/dl in the absence of identifiable secondary causes). Familial hypercholesterolemia (FH) phenotype was defined as a Dutch Lipid Clinic Network (DLCN) score ≥6. Participants underwent sequencing of LDLR, APOB, and PCSK9, and genotyping of 12 LDL-C-associated single-nucleotide variants to construct a polygenic score (PGS) for LDL-C. The presence of a pathogenic/likely pathogenic variant was considered monogenic etiology and a PGS ≥90th percentile was considered polygenic etiology. The mean LDL-C level was 187.3 ± 32.3 mg/dl and phenotypic FH was present in 8.4% of the cohort. An identifiable genetic etiology was present in 17.1% individuals (monogenic in 1.5% and polygenic in 15.6%). Phenotypic and genetic FH showed poor overlap. Only 26% of those who met the clinical criteria of FH had an identifiable genetic etiology and of those with an identifiable genetic etiology only 12.9% met clinical criteria for FH. Genetic factors explained 7.4% of the variance in LDL-C. In conclusion, in adults with primary hypercholesterolemia, 17.1% had an identifiable genetic etiology and the overlap between phenotypic and genetic FH was modest.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Virani SS, et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation. 2020;14:E139–E596. - PubMed
Grants and funding
- K24 HL137010/HL/NHLBI NIH HHS/United States
- K24-HL137010/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- R01 HL135879/HL/NHLBI NIH HHS/United States
- U01 HG006379/HG/NHGRI NIH HHS/United States
- U01HG006379/U.S. Department of Health & Human Services | NIH | National Human Genome Research Institute (NHGRI)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
