

Repurposing Immunomodulatory Imide Drugs (IMiDs) in Neuropsychiatric and Neurodegenerative Disorders
- PMID: 33854417
- PMCID: PMC8039148
- DOI: 10.3389/fnins.2021.656921
Repurposing Immunomodulatory Imide Drugs (IMiDs) in Neuropsychiatric and Neurodegenerative Disorders
Abstract
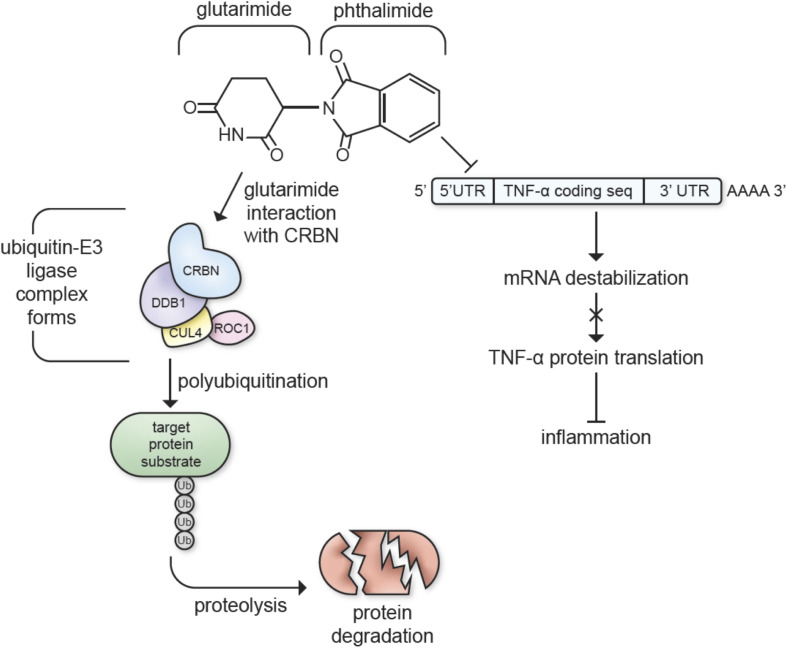
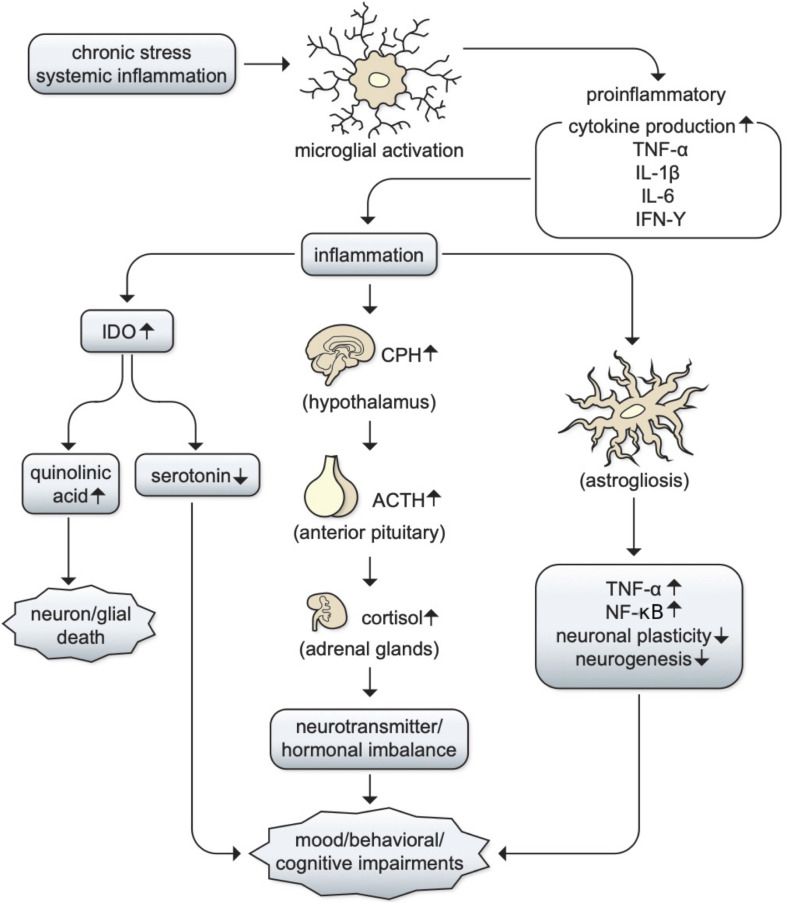
Neuroinflammation represents a common trait in the pathology and progression of the major psychiatric and neurodegenerative disorders. Neuropsychiatric disorders have emerged as a global crisis, affecting 1 in 4 people, while neurological disorders are the second leading cause of death in the elderly population worldwide (WHO, 2001; GBD 2016 Neurology Collaborators, 2019). However, there remains an immense deficit in availability of effective drug treatments for most neurological disorders. In fact, for disorders such as depression, placebos and behavioral therapies have equal effectiveness as antidepressants. For neurodegenerative diseases such as Parkinson's disease and Alzheimer's disease, drugs that can prevent, slow, or cure the disease have yet to be found. Several non-traditional avenues of drug target identification have emerged with ongoing neurological disease research to meet the need for novel and efficacious treatments. Of these novel avenues is that of neuroinflammation, which has been found to be involved in the progression and pathology of many of the leading neurological disorders. Neuroinflammation is characterized by glial inflammatory factors in certain stages of neurological disorders. Although the meta-analyses have provided evidence of genetic/proteomic upregulation of inflammatory factors in certain stages of neurological disorders. Although the mechanisms underpinning the connections between neuroinflammation and neurological disorders are unclear, and meta-analysis results have shown high sensitivity to factors such as disorder severity and sample type, there is significant evidence of neuroinflammation associations across neurological disorders. In this review, we summarize the role of neuroinflammation in psychiatric disorders such as major depressive disorder, generalized anxiety disorder, post-traumatic stress disorder, and bipolar disorder, as well as in neurodegenerative disorders, such as Parkinson's disease and Alzheimer's disease, and introduce current research on the potential of immunomodulatory imide drugs (IMiDs) as a new treatment strategy for these disorders.
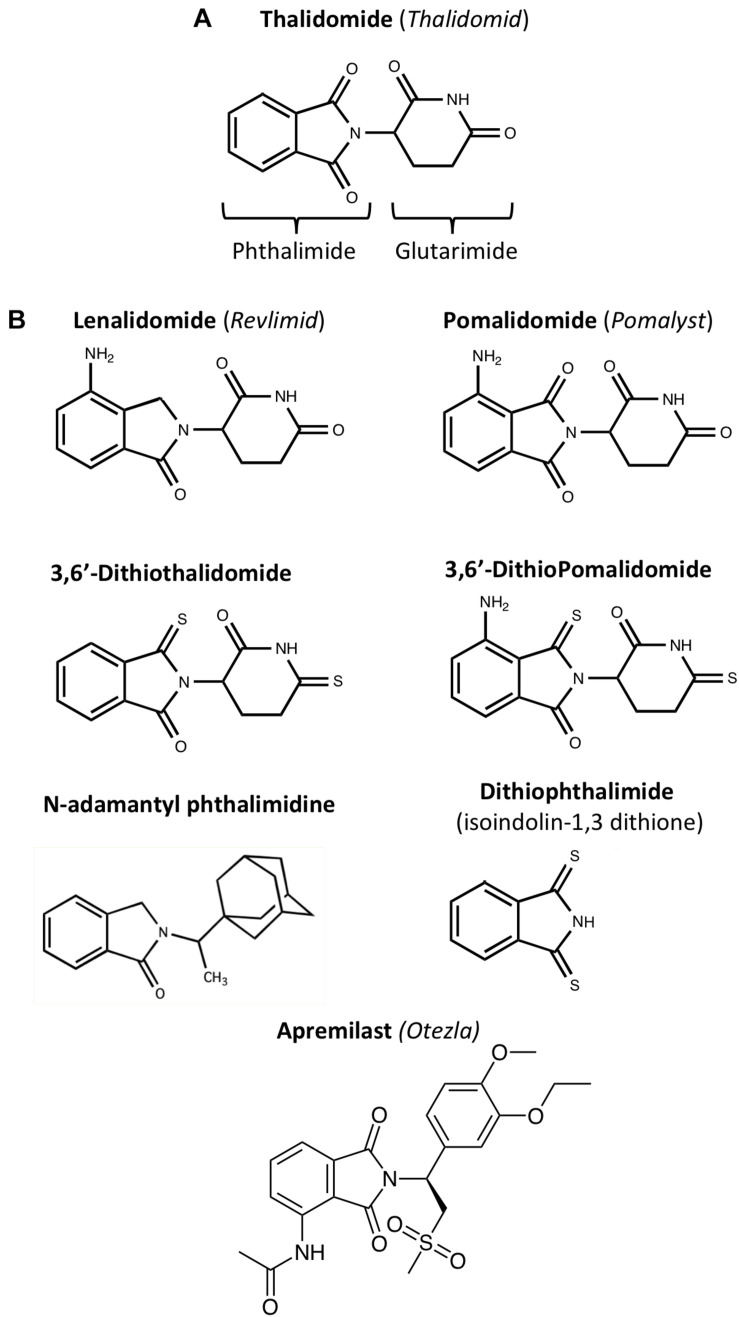
Keywords: IMiDs®; neurodegenarative diseases; neuroinflammation; neuropsychaitric disorders; pomalidomide; thalidomide.
Copyright © 2021 Jung, Tweedie, Scerba, Kim, Palmas, Pisanu, Carta and Greig.
Conflict of interest statement
DT and NG are named inventors on patents covering novel thalidomide analogs and have assigned all their rights to the National Institute on Aging, National Institutes of Health. DK was supported by the AevisBio (Gaithersburg, MD, United States and Daejeon, South Korea), a company with a research and development interest in treating neurodegenerative disorders, and an approved Cooperative Research and Development Agreement with NIA, NIH. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Activity of a Novel Anti-Inflammatory Agent F-3,6'-dithiopomalidomide as a Treatment for Traumatic Brain Injury.Biomedicines. 2022 Sep 30;10(10):2449. doi: 10.3390/biomedicines10102449. Biomedicines. 2022. PMID: 36289711 Free PMC article.
-
Neuroinflammation as a Factor of Neurodegenerative Disease: Thalidomide Analogs as Treatments.Front Cell Dev Biol. 2019 Dec 4;7:313. doi: 10.3389/fcell.2019.00313. eCollection 2019. Front Cell Dev Biol. 2019. PMID: 31867326 Free PMC article. Review.
-
A New Generation of IMiDs as Treatments for Neuroinflammatory and Neurodegenerative Disorders.Biomolecules. 2023 Apr 26;13(5):747. doi: 10.3390/biom13050747. Biomolecules. 2023. PMID: 37238617 Free PMC article. Review.
-
Dissecting the Relationship Between Neuropsychiatric and Neurodegenerative Disorders.Mol Neurobiol. 2023 Nov;60(11):6476-6529. doi: 10.1007/s12035-023-03502-9. Epub 2023 Jul 17. Mol Neurobiol. 2023. PMID: 37458987 Review.
-
Novel, thalidomide-like, non-cereblon binding drug tetrafluorobornylphthalimide mitigates inflammation and brain injury.J Biomed Sci. 2023 Mar 6;30(1):16. doi: 10.1186/s12929-023-00907-5. J Biomed Sci. 2023. PMID: 36872339 Free PMC article.
Cited by
-
Cancer drugs with high repositioning potential for Alzheimer's disease.Expert Opin Emerg Drugs. 2023 Dec;28(4):311-332. doi: 10.1080/14728214.2023.2296079. Epub 2023 Dec 26. Expert Opin Emerg Drugs. 2023. PMID: 38100555 Free PMC article. Review.
-
Thalidomide-induced limb malformations: an update and reevaluation.Arch Toxicol. 2025 May;99(5):1643-1747. doi: 10.1007/s00204-024-03930-z. Epub 2025 Apr 8. Arch Toxicol. 2025. PMID: 40198353 Review.
-
Activity of a Novel Anti-Inflammatory Agent F-3,6'-dithiopomalidomide as a Treatment for Traumatic Brain Injury.Biomedicines. 2022 Sep 30;10(10):2449. doi: 10.3390/biomedicines10102449. Biomedicines. 2022. PMID: 36289711 Free PMC article.
-
Comparative Genomics Identifies Putative Interspecies Mechanisms Underlying Crbn-Sall4-Linked Thalidomide Embryopathy.Front Genet. 2021 Jun 23;12:680217. doi: 10.3389/fgene.2021.680217. eCollection 2021. Front Genet. 2021. PMID: 34249098 Free PMC article.
-
3,6'-Dithiopomalidomide Ameliorates Hippocampal Neurodegeneration, Microgliosis and Astrogliosis and Improves Cognitive Behaviors in Rats with a Moderate Traumatic Brain Injury.Int J Mol Sci. 2021 Jul 31;22(15):8276. doi: 10.3390/ijms22158276. Int J Mol Sci. 2021. PMID: 34361041 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources