

Missing Insight Into T and B Cell Responses in Dermatitis Herpetiformis
- PMID: 33854513
- PMCID: PMC8039136
- DOI: 10.3389/fimmu.2021.657280
Missing Insight Into T and B Cell Responses in Dermatitis Herpetiformis
Abstract
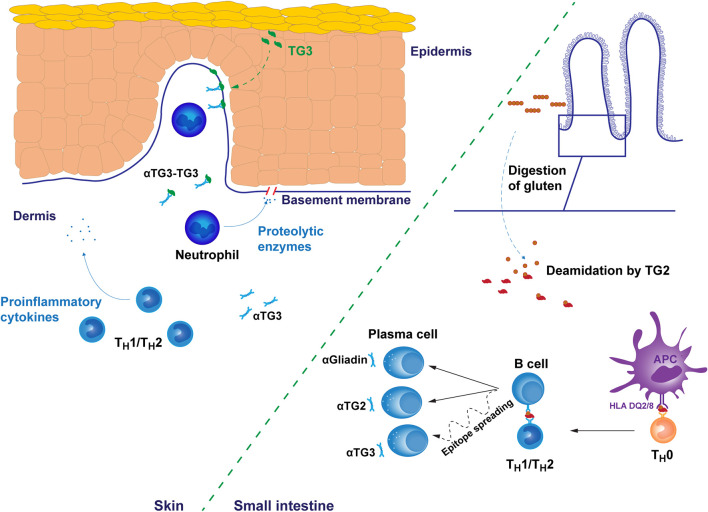
Dermatitis herpetiformis is a cutaneous form of celiac disease manifesting as an itching rash typically on the elbows, knees and buttocks. It is driven by the ingestion of gluten-containing cereals and characterized by granular deposits of immunoglobulin A in the papillary dermis. These antibodies target transglutaminase (TG) 3 and in the majority of patients they are also found in circulation. The circulating antibodies disappear and skin symptoms resolve as a result of gluten-free diet but the cutaneous anti-TG3 IgA deposits may persist for several years. In dermatitis herpetiformis, plasma cells secreting antibodies against TG3 are located in the intestinal mucosa similarly to those producing TG2 antibodies characteristic for celiac disease. In fact, both TG2- and TG3-specific plasma cells and gluten responsive T cells are found in dermatitis herpetiformis patients but the interplay between these cell populations is unknown. The small bowel mucosal damage in celiac disease is believed to be mediated by co-operation of cytotoxic intraepithelial T cells and the inflammatory milieu contributed by gluten-reactive CD4+ T cells, whereas the skin lesions in dermatitis herpetiformis appear to be devoid of gluten reactive T cells. Thus, how celiac disease-type intestinal T and B cell responses develop into an autoimmune condition affecting the skin is still incompletely understood. Finally, the skin and small bowel lesions may reappear upon reintroduction of gluten in patients treated with gluten-free diet but virtually nothing is known about the long-lived B cell and memory T cell populations activating in response to dietary gluten in dermatitis herpetiformis.
Keywords: B cell; T cell; celiac disease; dermatitis herpetiformis; epitope spreading; transglutaminase.
Copyright © 2021 Kemppainen, Salmi and Lindfors.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Antibody Responses to Transglutaminase 3 in Dermatitis Herpetiformis: Lessons from Celiac Disease.Int J Mol Sci. 2022 Mar 8;23(6):2910. doi: 10.3390/ijms23062910. Int J Mol Sci. 2022. PMID: 35328331 Free PMC article. Review.
-
Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease.Ann Med. 2017 Feb;49(1):23-31. doi: 10.1080/07853890.2016.1222450. Epub 2016 Dec 14. Ann Med. 2017. PMID: 27499257 Review.
-
Intestinal TG3- and TG2-Specific Plasma Cell Responses in Dermatitis Herpetiformis Patients Undergoing a Gluten Challenge.Nutrients. 2020 Feb 13;12(2):467. doi: 10.3390/nu12020467. Nutrients. 2020. PMID: 32069794 Free PMC article.
-
[Dermatitis herpetiformis].Tidsskr Nor Laegeforen. 2003 Nov 20;123(22):3234-6. Tidsskr Nor Laegeforen. 2003. PMID: 14714018 Norwegian.
-
[Dermatitis herpetiformis].Hautarzt. 2019 Apr;70(4):260-264. doi: 10.1007/s00105-019-4378-8. Hautarzt. 2019. PMID: 30868254 Review. German.
Cited by
-
Gluten Intolerance and Its Association With Skin Disorders: A Narrative Review.Cureus. 2023 Sep 1;15(9):e44549. doi: 10.7759/cureus.44549. eCollection 2023 Sep. Cureus. 2023. PMID: 37790051 Free PMC article. Review.
-
Antibody Responses to Transglutaminase 3 in Dermatitis Herpetiformis: Lessons from Celiac Disease.Int J Mol Sci. 2022 Mar 8;23(6):2910. doi: 10.3390/ijms23062910. Int J Mol Sci. 2022. PMID: 35328331 Free PMC article. Review.
-
The risk of renal comorbidities in celiac disease patients depends on the phenotype of celiac disease.J Intern Med. 2022 Nov;292(5):779-787. doi: 10.1111/joim.13532. Epub 2022 Jun 22. J Intern Med. 2022. PMID: 35713926 Free PMC article.
References
-
- Hietikko M, Hervonen K, Salmi T, Ilus T, Zone JJ, Kaukinen K, et al. . Disappearance of epidermal transglutaminase and IgA deposits from the papillary dermis of patients with dermatitis herpetiformis after a long-term gluten-free diet. Br J Dermatol (2018) 178:e198–201. 10.1111/bjd.15995 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous