

Quadrigeminal cistern arachnoid cyst as a probable cause of hemifacial spasm
- PMID: 33854668
- PMCID: PMC8026915
- DOI: 10.1016/j.radcr.2021.02.061
Quadrigeminal cistern arachnoid cyst as a probable cause of hemifacial spasm
Erratum in
-
Erratum regarding missing patient consent statements in previously published articles.Radiol Case Rep. 2023 Jan 20;18(3):1383-1384. doi: 10.1016/j.radcr.2022.10.047. eCollection 2023 Mar. Radiol Case Rep. 2023. PMID: 36818994 Free PMC article.
Abstract
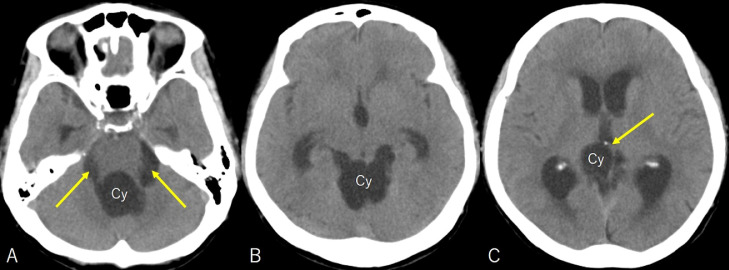
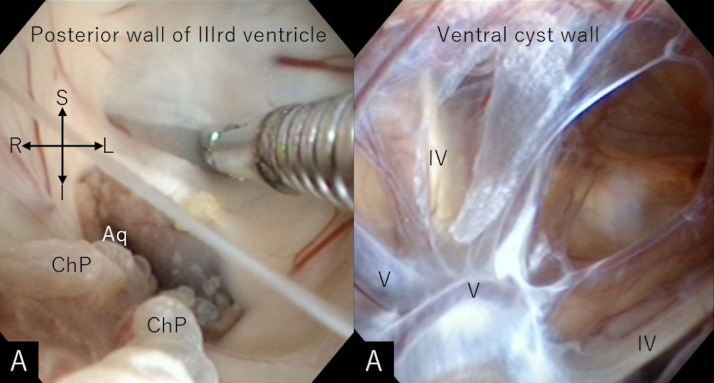
Arachnoid cysts arising in the quadrigeminal cistern (ACQCs) are uncommon. A 68-year-old woman presented with an unsteady gait, facial spasm, and cerebellar ataxia. Non-contrast head computed tomography showed a cystic mass centered in the quadrigeminal cistern accompanying ventriculomegaly. On MRI, the cyst appeared hypointense on T1- and hyperintense on T2-weighted sequence. There was no restricted diffusion on diffusion-weighted imaging. The cerebral aqueduct was obstructed and the prepontine cistern was narrowed. The left vertebral artery (VA) coursed adjacent to the facial nerve at its origin. The patient underwent neuroendoscopic fenestration of the posterior wall of the third ventricle and ventral wall of the ACQC. Postoperatively, the patient's symptoms resolved. MRI showed a considerable reduction in the ACQC and expansion of the prepontine cistern, whereas the relationship between the left VA and the proximal segment of the facial nerve did not change. We assumed that the pre-existing close relationship between the VA and facial nerve might have been aggravated by the anterior displacement of the brainstem, thus causing the facial spasm.
Keywords: Arachnoid cyst; Endoscopic fenestration; Hemifacial spasm; Quadrigeminal cistern.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
-
- Garg K, Tandon V, Sharma S, Suri A, Chandra PS, Kumar R. Quadrigeminal cistern arachnoid cyst: a series of 18 patients and a review of literature. Br J Neurosurg. 2015;29:70–76. - PubMed
-
- Basauri L, Selman JM. Intracranial arachnoidal cysts. Childs Nerv Syst. 1992;8:101–104. - PubMed
-
- Cinalli G, Spennato P, Columbano L, Ruggiero C, Aliberti F, Trischitta V. Neuroendoscopic treatment of arachnoid cysts of the quadrigeminal cistern: a series of 14 cases. J Neurosurg Pediatr. 2010;6:489–497. - PubMed
-
- Deopujari CE, Shaikh ST, Karmarkar VS, Sudha AY, Mohanty CB, Biyani NK. Experience with management of intracranial arachnoid cysts. J Neurol Surg A Cent Eur Neurosurg. 2012;82:43–52. - PubMed
-
- Inamasu J, Ohira T, Nakamura Y, Saito R, Kuroshima Y, Mayanagi K. Endoscopic ventriculo-cystomy for non-communicating hydrocephalus secondary to quadrigeminal cistern arachnoid cyst. Acta Neurol Scand. 2003;107:67–71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
