

The effect of preoperative embolization on surgical outcomes for carotid body tumor resection
- PMID: 33854776
- PMCID: PMC8013905
- DOI: 10.1177/20503121211005229
The effect of preoperative embolization on surgical outcomes for carotid body tumor resection
Abstract
Objective: Compare the effects of preoperative embolization for carotid body tumor resection on surgical outcomes to carotid body tumor resections without preoperative embolization.
Methods: Single-center retrospective review of all consecutive patients who underwent carotid body tumor resection from 2001 to 2019. Surgical outcomes with emphasis on operative time (estimated blood loss and cranial nerve injury) of patients undergoing carotid body tumor resection following preoperative embolization were compared to those undergoing resection alone using unpaired Student's t-test and Fisher's exact test.
Results: Forty-six patients (15% male, mean age 50 ± 15 years) underwent resection of 49 carotid body tumors. Patients undergoing preoperative embolization (n = 20 (40%)) had larger mean tumor size (4.0 ± 0.7 vs 3.2 ± 1 cm, p = 0.006), increased Shamblin II/III tumor classification (18 (90%) vs 22 (76%), p < 0.001), operative time (337 ± 195 vs 199 ± 100 min, p = 0.004), and cranial nerve injuries overall (8 (40%) vs 2 (10%), p = 0.01) compared to patients undergoing resection without preoperative embolization (n = 29 (60%)). In subgroup analysis of Shamblin II/III classification tumors (n = 40), preoperative embolization (n = 18) was associated with increased tumor size (4.1 ± 0.6 vs 3.5 ± 0.9 cm, p = 0.01), operative time (351 ± 191 vs 244 ± 105 min, p = 0.02), and cranial nerve injury overall (8 (44%) vs 2 (9%), p = 0.03) compared to resections alone (n = 19). In further subgroup analysis of large (⩾ 3 cm) tumors (n = 37), preoperative embolization (n = 18) was associated with increased operative time (350 ± 191 vs 198 ± 99 min, p = 0.006) and cranial nerve injury overall (8 (44%) vs 2 (11%), p = 0.03) compared to resections alone (n = 19). There were no significant differences in estimated blood loss, transfusion requirement, or hematoma formation between any of the embolization and non-embolization subgroups.
Conclusion: After controlling for tumor Shamblin classification and size, carotid body tumor resections following preoperative embolization were associated with increased operative time and inferior surgical outcomes compared to those tumors undergoing resection alone. Nonetheless, such results remain susceptible to the confounding effects of individual tumor characteristics often used in the decision to perform preoperative embolization, underscoring the need for prospective studies evaluating the utility of preoperative embolization for carotid body tumors.
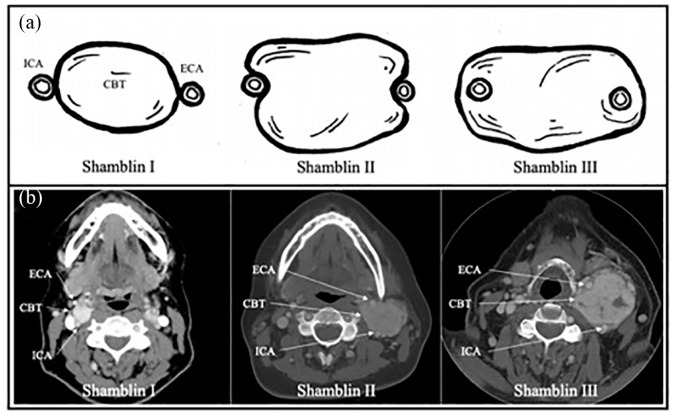
Keywords: Carotid body tumor; Shamblin classification; cranial nerve injury; high-altitude; preoperative embolization.
© The Author(s) 2021.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Robertson V, Poli F, Hobson B, et al.. A systematic review and meta-analysis of the presentation and surgical management of patients with carotid body tumours. Eur J Vasc Endovasc Surg 2019; 57(4): 477–486. - PubMed
-
- Sajid MS, Hamilton G, Baker DM, et al.. A multicenter review of carotid body tumour management. Eur J Vasc Endovasc Surg 2007; 34(2): 127–130. - PubMed
-
- Davila VJ, Chang JM, Stone WM, et al.. Current surgical management of carotid body tumors. J Vasc Surg 2016; 64(6): 1703–1710. - PubMed
-
- Nora JD, Hallett JW, O’Brien PC, et al.. Surgical resection of carotid body tumors: long-term survival, recurrence, and metastasis. Mayo Clin Proc 1988; 63: 348–352. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
