

Association of Routinely Measured Proinflammatory Biomarkers With Abnormal MRI Findings in Asphyxiated Neonates Undergoing Therapeutic Hypothermia
- PMID: 33855004
- PMCID: PMC8039151
- DOI: 10.3389/fped.2021.624652
Association of Routinely Measured Proinflammatory Biomarkers With Abnormal MRI Findings in Asphyxiated Neonates Undergoing Therapeutic Hypothermia
Abstract
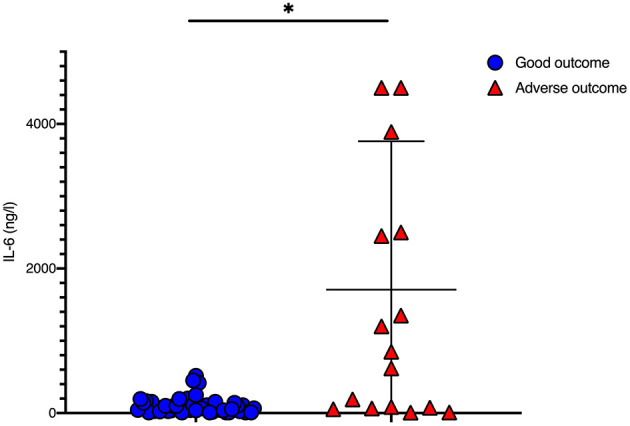
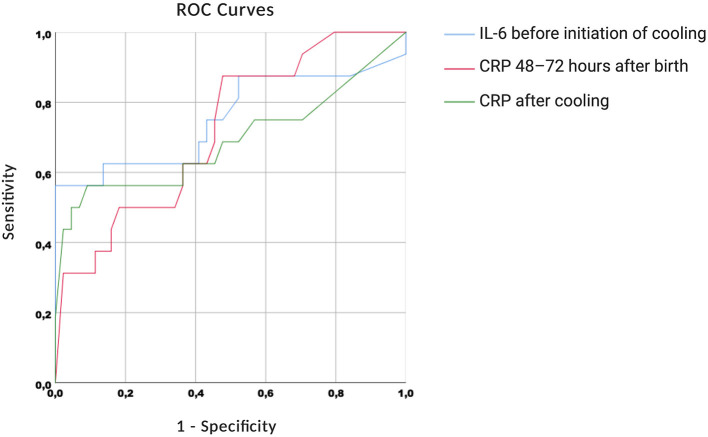
Background: The neuroprotective treatment effect of therapeutic hypothermia (TH) following perinatal asphyxia may be negatively influenced by neonatal sepsis and concomitant inflammation. We aimed to correlate routinely used blood biomarkers for perinatal sepsis in cooled asphyxiated newborns with MRI findings. Methods: Perinatal data was retrospectively collected from 67 cooled asphyxiated newborns. Levels of C-reactive protein (CRP), white blood cells and platelets were analyzed before, during and after TH. Interleukin-6 blood levels were analyzed before initiation of TH. Magnetic resonance imaging (MRI) on postnatal day 5-7 was used defining short-term outcome. Adverse outcome was defined as death or adverse MRI findings. Amplitude-integrated electroencephalography (aEEG) was additionally analyzed and correlated with short-term MRI outcome. Results: Forty-nine newborns had favorable short-term MRI outcome. Perinatal data referring to perinatal sepsis did not differ significantly between groups. IL-6 levels before initiation of TH and CRP levels on day three and after TH were significantly higher in newborns with adverse short-term MRI outcome. Males with adverse short-term MRI outcome had significantly increased CRP values at the end of the cooling phase. aEEG strongly correlated with short-term MRI outcome. Conclusion: Routinely used blood biomarkers may be helpful early identifying newborns at high risk of unfavorable outcome and in need of close neurodevelopmental follow-up.
Keywords: aEEG; asphyxia; biomarker; cooling; newborn; outcome.
Copyright © 2021 Ruhfus, Giannakis, Markus, Stein, Hoehn, Felderhoff-Mueser and Sabir.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Mechanical Ventilation, Partial Pressure of Carbon Dioxide, Increased Fraction of Inspired Oxygen and the Increased Risk for Adverse Short-Term Outcomes in Cooled Asphyxiated Newborns.Children (Basel). 2021 May 21;8(6):430. doi: 10.3390/children8060430. Children (Basel). 2021. PMID: 34063852 Free PMC article.
-
Towards multimodal brain monitoring in asphyxiated newborns with amplitude-integrated EEG and simultaneous somatosensory evoked potentials.Early Hum Dev. 2021 Feb;153:105287. doi: 10.1016/j.earlhumdev.2020.105287. Epub 2020 Dec 2. Early Hum Dev. 2021. PMID: 33310460
-
Early Imaging and Adverse Neurodevelopmental Outcome in Asphyxiated Newborns Treated With Hypothermia.Pediatr Neurol. 2017 Aug;73:20-27. doi: 10.1016/j.pediatrneurol.2017.04.025. Epub 2017 May 19. Pediatr Neurol. 2017. PMID: 28619376
-
Prediction of outcome methods assessing short- and long-term outcome after therapeutic hypothermia.Semin Fetal Neonatal Med. 2015 Apr;20(2):115-21. doi: 10.1016/j.siny.2014.10.006. Epub 2014 Nov 1. Semin Fetal Neonatal Med. 2015. PMID: 25457081 Review.
-
Hypothermia therapy for newborns with hypoxic ischemic encephalopathy.J Pediatr (Rio J). 2015 Nov-Dec;91(6 Suppl 1):S78-83. doi: 10.1016/j.jped.2015.07.004. Epub 2015 Sep 4. J Pediatr (Rio J). 2015. PMID: 26354871 Review.
Cited by
-
Additive Impact of Interleukin 6 and Neuron Specific Enolase for Prognosis in Patients With Out-of-Hospital Cardiac Arrest - Experience From the HAnnover COoling REgistry.Front Cardiovasc Med. 2022 May 31;9:899583. doi: 10.3389/fcvm.2022.899583. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35711345 Free PMC article.
-
Evaluating of neonatal early onset sepsis through lactate and base excess monitoring.Sci Rep. 2023 Sep 8;13(1):14837. doi: 10.1038/s41598-023-41776-0. Sci Rep. 2023. PMID: 37684308 Free PMC article.
-
The Impact of Time to Initiate Therapeutic Hypothermia on Short-Term Neurological Outcomes in Neonates with Hypoxic-Ischemic Encephalopathy.Children (Basel). 2024 Jun 4;11(6):686. doi: 10.3390/children11060686. Children (Basel). 2024. PMID: 38929265 Free PMC article.
-
Mechanical Ventilation, Partial Pressure of Carbon Dioxide, Increased Fraction of Inspired Oxygen and the Increased Risk for Adverse Short-Term Outcomes in Cooled Asphyxiated Newborns.Children (Basel). 2021 May 21;8(6):430. doi: 10.3390/children8060430. Children (Basel). 2021. PMID: 34063852 Free PMC article.
-
Fluid Supply and Feeding Practices in Cooled Asphyxiated Newborns.Children (Basel). 2021 Oct 9;8(10):899. doi: 10.3390/children8100899. Children (Basel). 2021. PMID: 34682164 Free PMC article.
References
-
- Basu SK, Kaiser JR, Guffey D, Minard CG, Guillet R, Gunn AJ. Hypoglycaemia and hyperglycaemia are associated with unfavourable outcome in infants with hypoxic ischaemic encephalopathy: a post hoc analysis of the CoolCap Study. Arch Dis Child Fetal Neonatal Ed. (2016) 101:F149–55. 10.1136/archdischild-2015-308733 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous