

Carvedilol prevents impairment of the counterregulatory response in recurrently hypoglycaemic diabetic rats
- PMID: 33855225
- PMCID: PMC8029566
- DOI: 10.1002/edm2.226
Carvedilol prevents impairment of the counterregulatory response in recurrently hypoglycaemic diabetic rats
Abstract
Aim: It has been suggested that repeated activation of the adrenergic system during antecedent episodes of hypoglycaemia contributes to the development of counterregulatory failure. We previously reported that treatment with carvedilol, a non-specific β-blocker, prevented the development of counterregulatory failure and improved hypoglycaemia awareness in recurrently hypoglycaemic non-diabetic rats. The current study investigated whether carvedilol has similar benefits in diabetic rats.
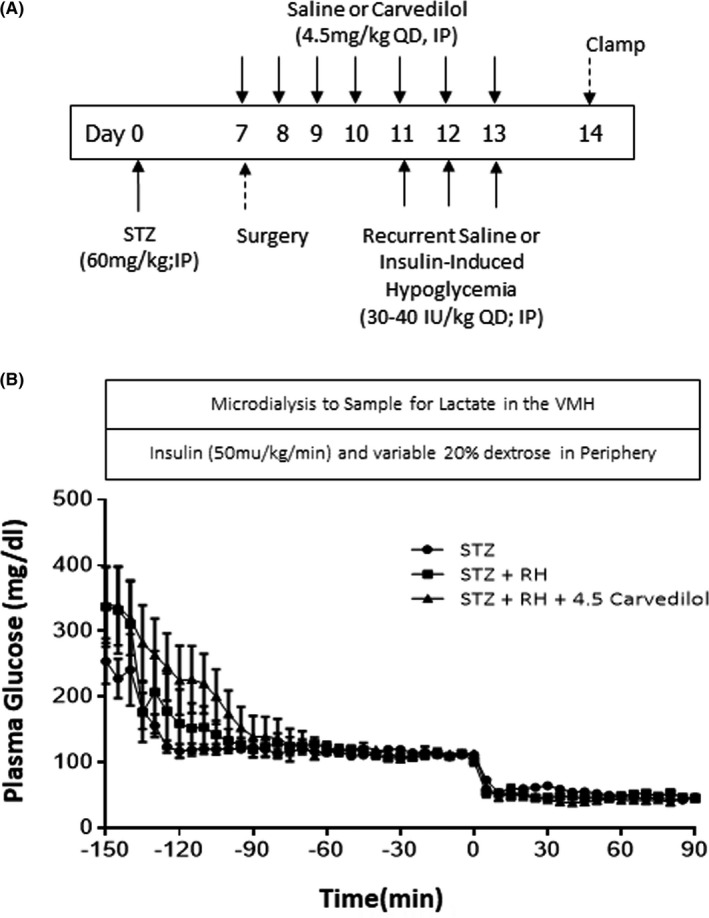
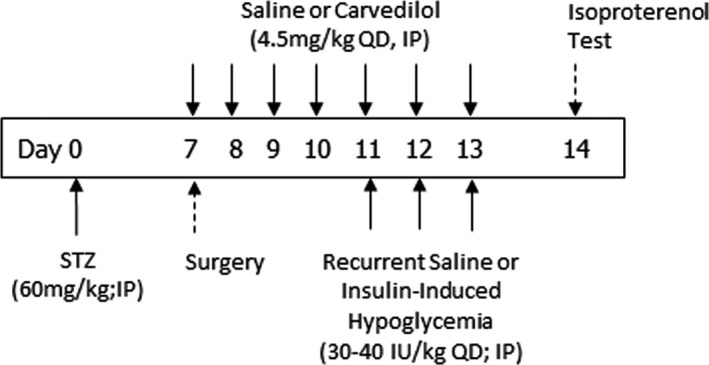
Methods: Recurrently hypoglycaemic streptozotocin-diabetic rats (STZ+RH) were treated with carvedilol for one week prior to undergoing a hypoglycaemic clamp. Hypoglycaemia awareness was evaluated in streptozotocin-diabetic rats made hypoglycaemia unaware using repeated injections of 2-deoxyglucose.
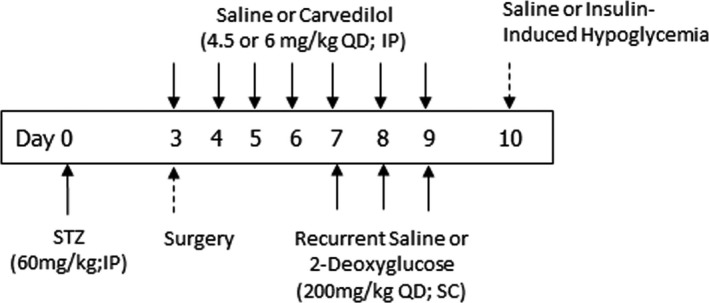
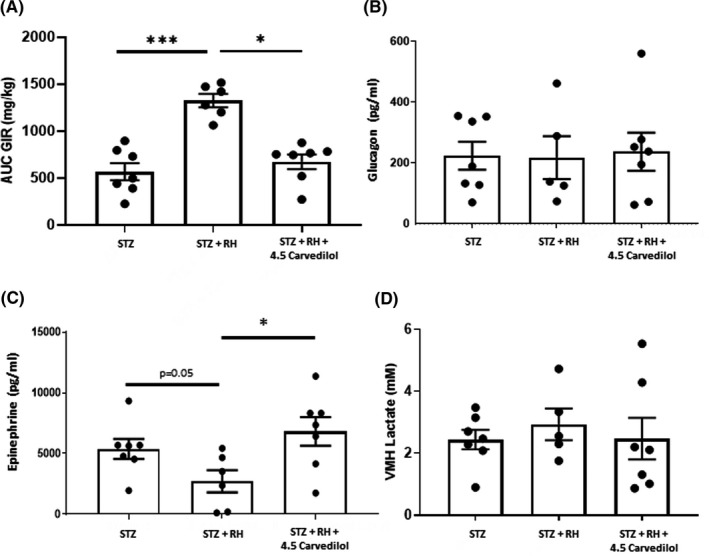
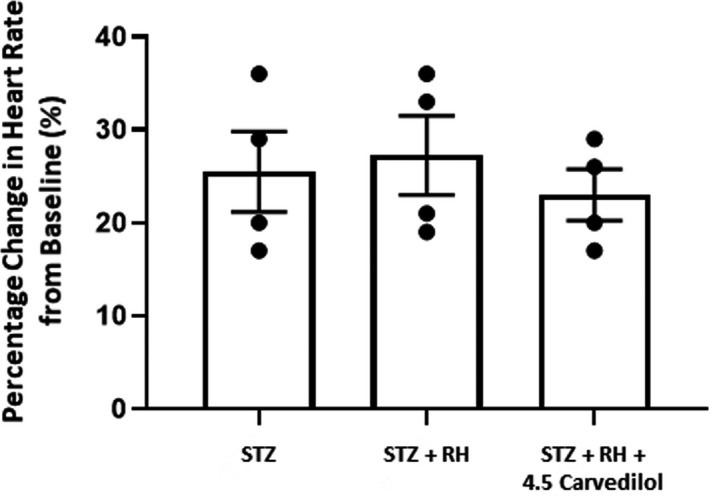
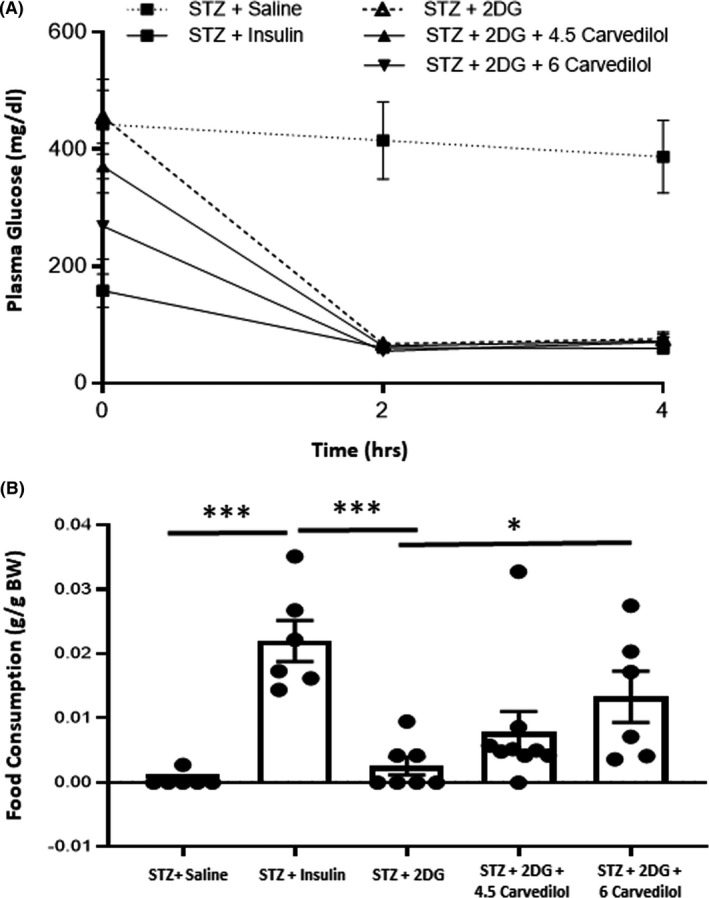
Results: Compared to hypoglycaemia-naïve STZ-diabetic controls, exogenous glucose requirements were more than doubled in the STZ+RH animals and this was associated with a 49% reduction in the epinephrine response to hypoglycaemia. Treating STZ+RH animals with carvedilol improved the epinephrine response to hypoglycaemia. Of note, neither recurrent hypoglycaemia nor carvedilol treatment affected the glucagon response in diabetic animals. Additionally, carvedilol treatment improved the feeding response to insulin-induced hypoglycaemia in diabetic animals made 'hypoglycaemia unaware' using repeated injections of 2-deoxyglucose, suggesting the treatment improved awareness of hypoglycaemia as well.
Conclusion: Our data suggest that carvedilol may be useful in preventing impairments of the sympathoadrenal response and the development of hypoglycaemia unawareness during recurring episodes of hypoglycaemia in diabetic animals.
Keywords: adrenergic sensitivity; beta‐blocker; carvedilol; diabetes; hypoglycaemia; hypoglycaemia awareness; streptozotocin.
© 2021 The Authors. Endocrinology, Diabetes & Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
Carvedilol prevents counterregulatory failure and impaired hypoglycaemia awareness in non-diabetic recurrently hypoglycaemic rats.Diabetologia. 2019 Apr;62(4):676-686. doi: 10.1007/s00125-018-4802-0. Epub 2019 Jan 9. Diabetologia. 2019. PMID: 30627753 Free PMC article.
-
Effects of insulin treatment without and with recurrent hypoglycemia on hypoglycemic counterregulation and adrenal catecholamine-synthesizing enzymes in diabetic rats.Endocrinology. 2006 Apr;147(4):1860-70. doi: 10.1210/en.2005-1040. Epub 2006 Jan 5. Endocrinology. 2006. PMID: 16396986
-
Unawareness of hypoglycaemia and inadequate hypoglycaemic counterregulation: no causal relation with diabetic autonomic neuropathy.BMJ. 1990 Oct 6;301(6755):783-7. doi: 10.1136/bmj.301.6755.783. BMJ. 1990. PMID: 2224265 Free PMC article.
-
Drug-induced disorders of glucose metabolism. Mechanisms and management.Drug Saf. 1996 Aug;15(2):135-57. doi: 10.2165/00002018-199615020-00005. Drug Saf. 1996. PMID: 8884164 Review.
-
Pathophysiology and management of recurrent hypoglycaemia and hypoglycaemia unawareness in diabetes.Neth J Med. 2006 Sep;64(8):269-79. Neth J Med. 2006. PMID: 16990690 Review.
Cited by
-
Glucagon-like peptide-1 and impaired counterregulatory responses to hypoglycemia in type 1 diabetes.World J Diabetes. 2025 Feb 15;16(2):99928. doi: 10.4239/wjd.v16.i2.99928. World J Diabetes. 2025. PMID: 39959274 Free PMC article.
-
Effects of Carvedilol on Blood Pressure, Blood Sugar, and Blood Lipids in Elderly Patients with Refractory Hypertension.Comput Math Methods Med. 2022 Jul 27;2022:7889024. doi: 10.1155/2022/7889024. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Sep 27;2023:9867142. doi: 10.1155/2023/9867142. PMID: 35936366 Free PMC article. Retracted.
-
Experimental pharmacological approaches to reverse impaired awareness of hypoglycemia-a review.Front Pharmacol. 2024 Jan 23;15:1349004. doi: 10.3389/fphar.2024.1349004. eCollection 2024. Front Pharmacol. 2024. PMID: 38323079 Free PMC article. Review.
-
Current and future therapies to treat impaired awareness of hypoglycemia.Front Pharmacol. 2023 Oct 24;14:1271814. doi: 10.3389/fphar.2023.1271814. eCollection 2023. Front Pharmacol. 2023. PMID: 37942482 Free PMC article. Review.
-
Role of the Adrenal Medulla in Hypoglycaemia-Associated Autonomic Failure-A Diabetic Perspective.Metabolites. 2024 Jan 31;14(2):100. doi: 10.3390/metabo14020100. Metabolites. 2024. PMID: 38392992 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
