

Cervicogenic dizziness alleviation after coblation discoplasty: a retrospective study
- PMID: 33855907
- PMCID: PMC8057077
- DOI: 10.1080/07853890.2021.1910336
Cervicogenic dizziness alleviation after coblation discoplasty: a retrospective study
Abstract
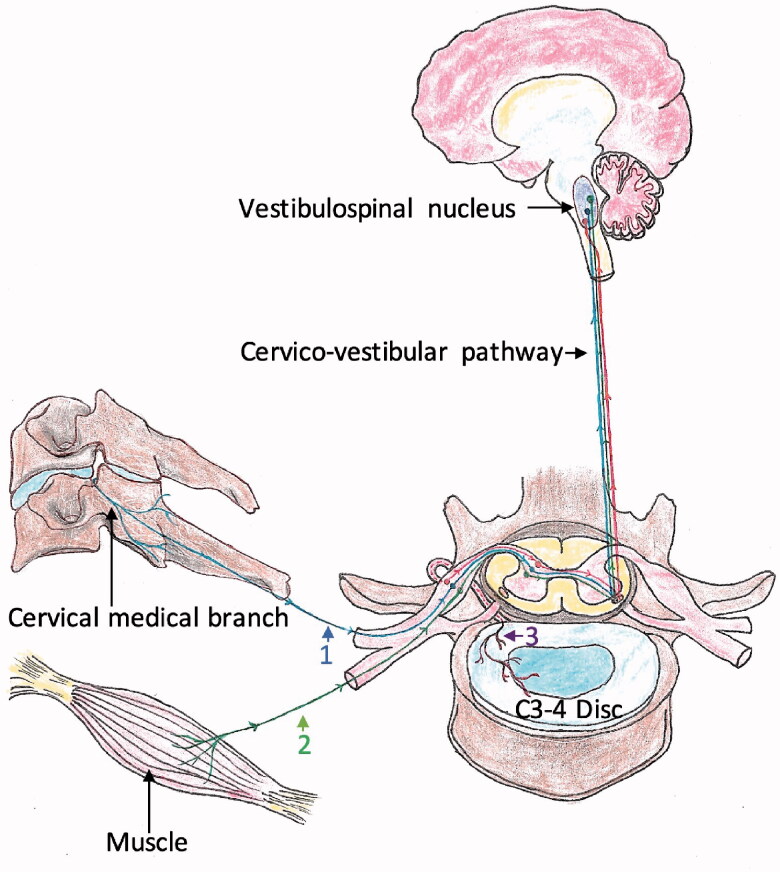
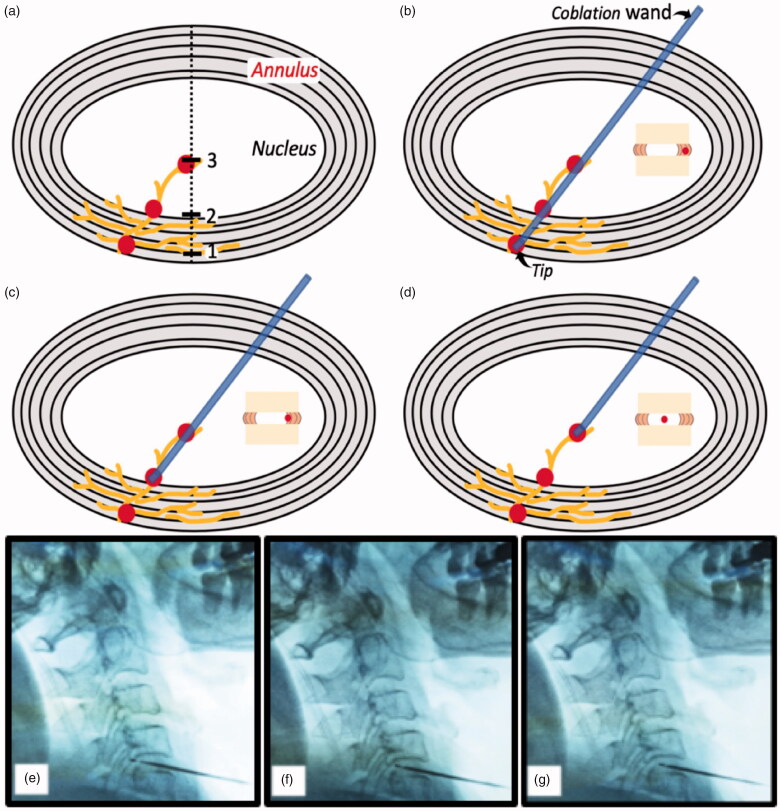
Objective: Little is known about the therapeutic relationship between coblation discoplasty and cervicogenic dizziness (CGD). CGD can be caused by abnormal proprioceptive inputs from compressed nerve roots, intradiscal mechanoreceptors and nociceptors to the vestibulospinal nucleus in the degenerative cervical disc. The aim was to analyze the efficacy of coblation discoplasty in CGD through intradiscal nerve ablation and disc decompression in a 12-month follow-up retrospective study.
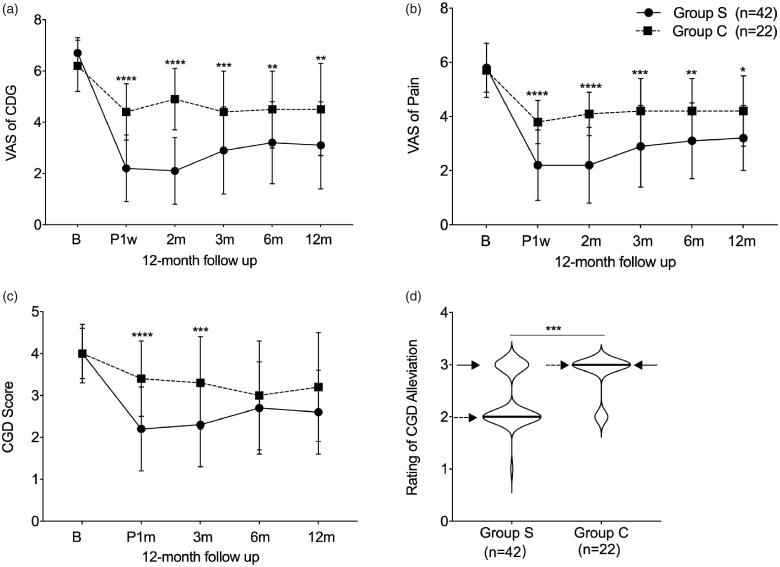
Methods: From 2015 to 2019, 42 CGD patients who received coblation discolplasty were recruited as the surgery group, and 22 CGD patients who rejected surgery were recruited as the conservative group. Using intent-to-treat (ITT) analysis, we retrospectively analyzed the CGD visual analogue scale (VAS), neck pain VAS, CGD frequency score, and the CGD alleviation rating throughout a 12-month follow-up period.
Results: Compared with conservative intervention, coblation discoplasty revealed a better recovery trend with effect sizes of 1.76, 2.15, 0.92, 0.78 and 0.81 in CGD VAS, and effect sizes of 1.32, 1.54, 0.93, 0.86 and 0.76in neck pain VAS at post-operative 1 week, and 1, 3, 6, 12 months, respectively. The lower CGD frequency score indicated fewer attacks of dizziness until postoperative 3 months (p < 0.01). At post-operative 12 months, the coblation procedure showed increased satisfactory outcomes of CGD alleviation rating (p < .001, -1.00 of effect size).
Conclusions: Coblation discoplasty significantly improves the severity and frequency of CGD, which is important inbridging unresponsive conservative intervention and open surgery.Key messagesThere is a correlation between the degenerative cervical disc and cervicogenic dizziness (CGD).CGD can be caused by abnormal proprioceptive inputs from a compressed nerve root and intradiscal mechanoreceptors and nociceptors to the vestibulospinal nucleus in the degenerative cervical disc.Cervical coblation discoplasty can alleviate CGD through ablating intradiscal nerve endings and decompressing the nerve root.
Keywords: Cervicogenic dizziness; cervicogenic vertigo; coblation discoplasty; coblation nucleoplasty.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Jung FC, Mathew S, Littmann AE, et al. Clinical decision making in the management of patients with cervicogenic dizziness: a case series. J Orthop Sports Phys Ther. 2017;47(11):874–884. - PubMed
-
- Bisdorff A, Von Brevern M, Lempert T, et al. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res. 2009;19(1–2):1–13. - PubMed
-
- Devaraja K. Approach to cervicogenic dizziness: a comprehensive review of its aetiopathology and management. Eur Arch Otorhinolaryngol. 2018;275(10):2421–2433. - PubMed
-
- Bankoul S, Goto T, Yates B, et al. Cervical primary afferent input to vestibulospinal neurons projecting to the cervical dorsal horn: an anterograde and retrograde tracing study in the cat. J Comp Neurol. 1995;353(4):529–538. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical