

COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital
- PMID: 33856027
- PMCID: PMC8083258
- DOI: 10.1093/brain/awab148
COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital
Abstract
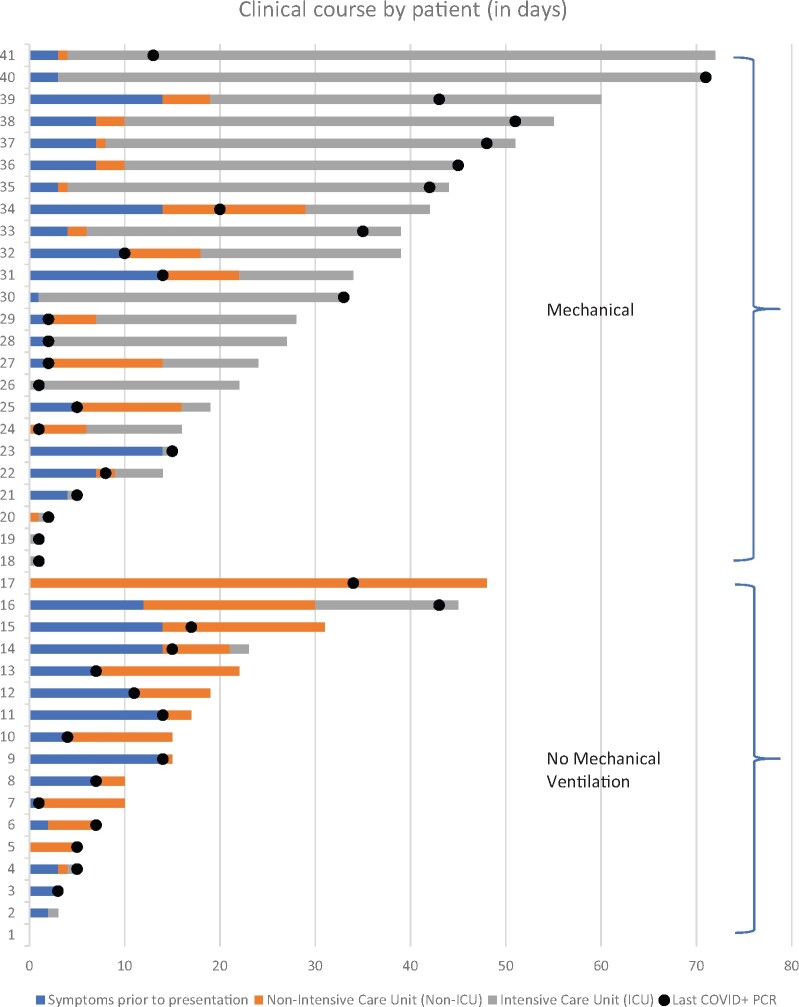
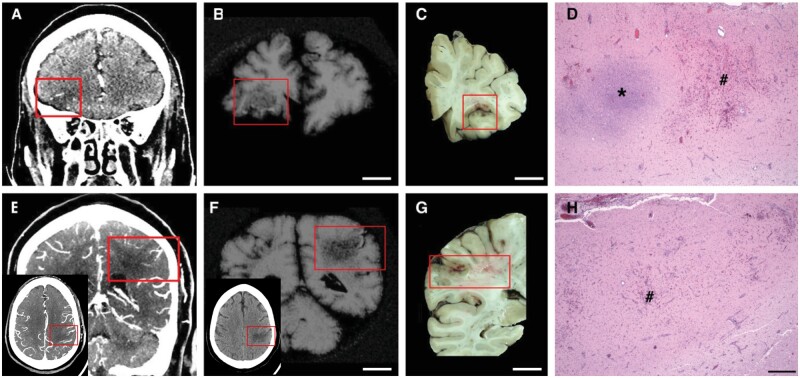
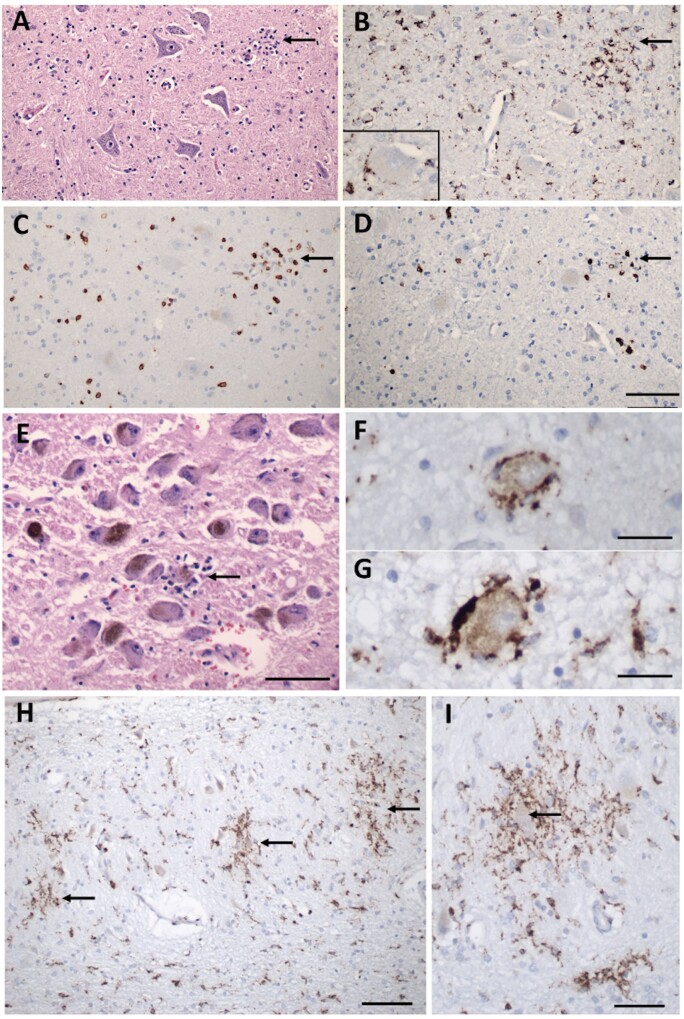
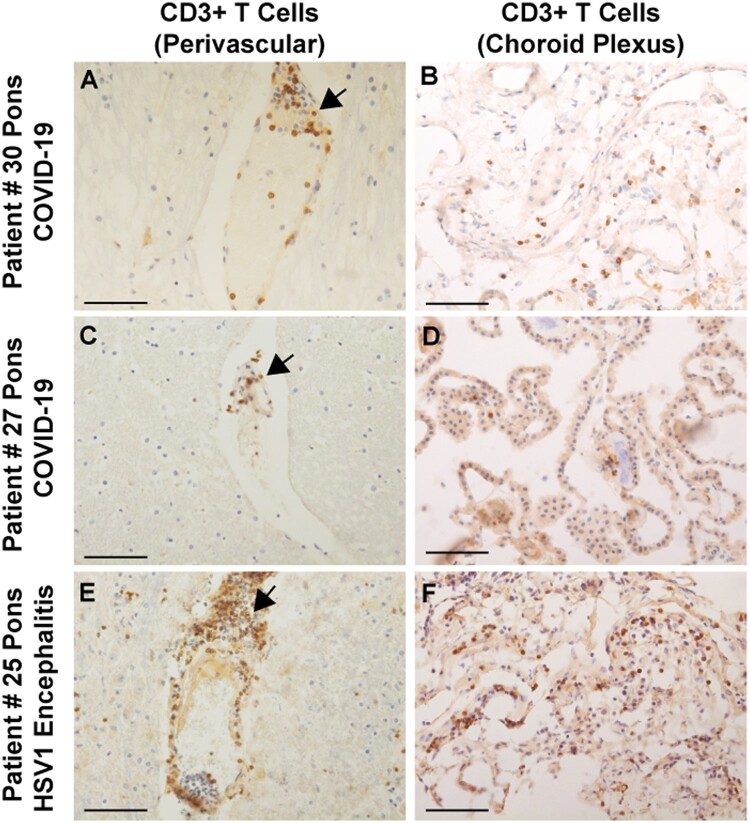
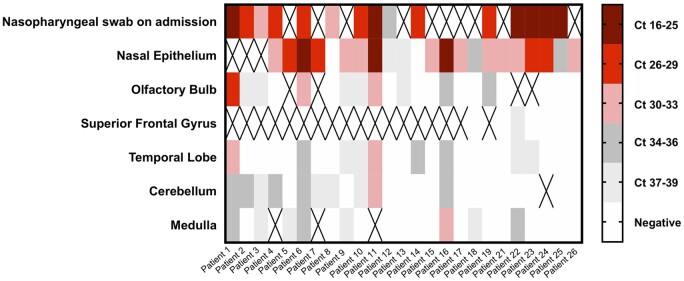
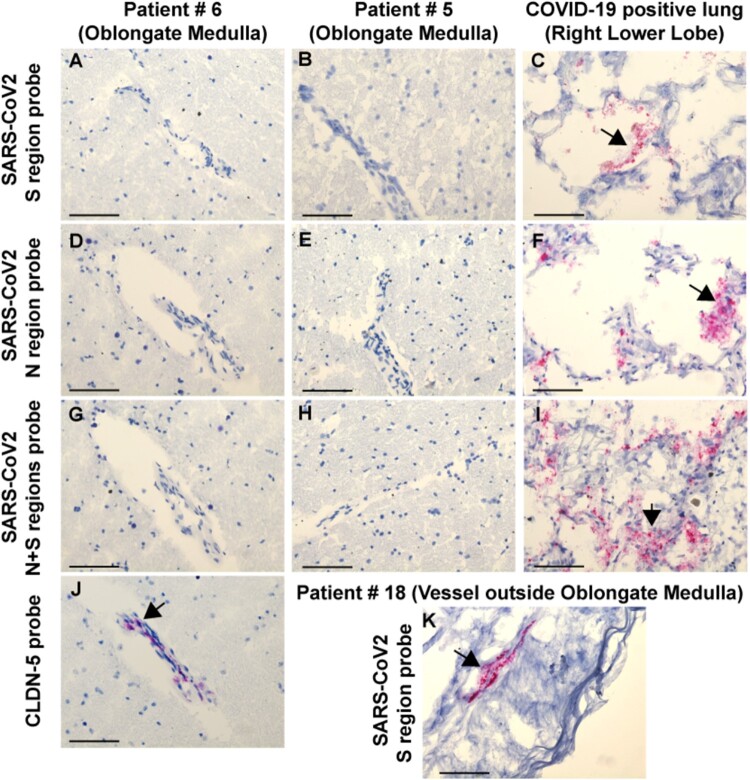
Many patients with SARS-CoV-2 infection develop neurological signs and symptoms; although, to date, little evidence exists that primary infection of the brain is a significant contributing factor. We present the clinical, neuropathological and molecular findings of 41 consecutive patients with SARS-CoV-2 infections who died and underwent autopsy in our medical centre. The mean age was 74 years (38-97 years), 27 patients (66%) were male and 34 (83%) were of Hispanic/Latinx ethnicity. Twenty-four patients (59%) were admitted to the intensive care unit. Hospital-associated complications were common, including eight patients (20%) with deep vein thrombosis/pulmonary embolism, seven (17%) with acute kidney injury requiring dialysis and 10 (24%) with positive blood cultures during admission. Eight (20%) patients died within 24 h of hospital admission, while 11 (27%) died more than 4 weeks after hospital admission. Neuropathological examination of 20-30 areas from each brain revealed hypoxic/ischaemic changes in all brains, both global and focal; large and small infarcts, many of which appeared haemorrhagic; and microglial activation with microglial nodules accompanied by neuronophagia, most prominently in the brainstem. We observed sparse T lymphocyte accumulation in either perivascular regions or in the brain parenchyma. Many brains contained atherosclerosis of large arteries and arteriolosclerosis, although none showed evidence of vasculitis. Eighteen patients (44%) exhibited pathologies of neurodegenerative diseases, which was not unexpected given the age range of our patients. We examined multiple fresh frozen and fixed tissues from 28 brains for the presence of viral RNA and protein, using quantitative reverse-transcriptase PCR, RNAscope® and immunocytochemistry with primers, probes and antibodies directed against the spike and nucleocapsid regions. The PCR analysis revealed low to very low, but detectable, viral RNA levels in the majority of brains, although they were far lower than those in the nasal epithelia. RNAscope® and immunocytochemistry failed to detect viral RNA or protein in brains. Our findings indicate that the levels of detectable virus in coronavirus disease 2019 brains are very low and do not correlate with the histopathological alterations. These findings suggest that microglial activation, microglial nodules and neuronophagia, observed in the majority of brains, do not result from direct viral infection of brain parenchyma, but more likely from systemic inflammation, perhaps with synergistic contribution from hypoxia/ischaemia. Further studies are needed to define whether these pathologies, if present in patients who survive coronavirus disease 2019, might contribute to chronic neurological problems.
Keywords: COVID-19; SARS-CoV-2; microglia activation; microglial nodules; neuropathology.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Nath A. Neurologic complications of coronavirus infections. Neurology. 2020;94(19):809–810. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
