

Clinical Applications of Dual-Energy CT
- PMID: 33856133
- PMCID: PMC8154785
- DOI: 10.3348/kjr.2020.0996
Clinical Applications of Dual-Energy CT
Abstract
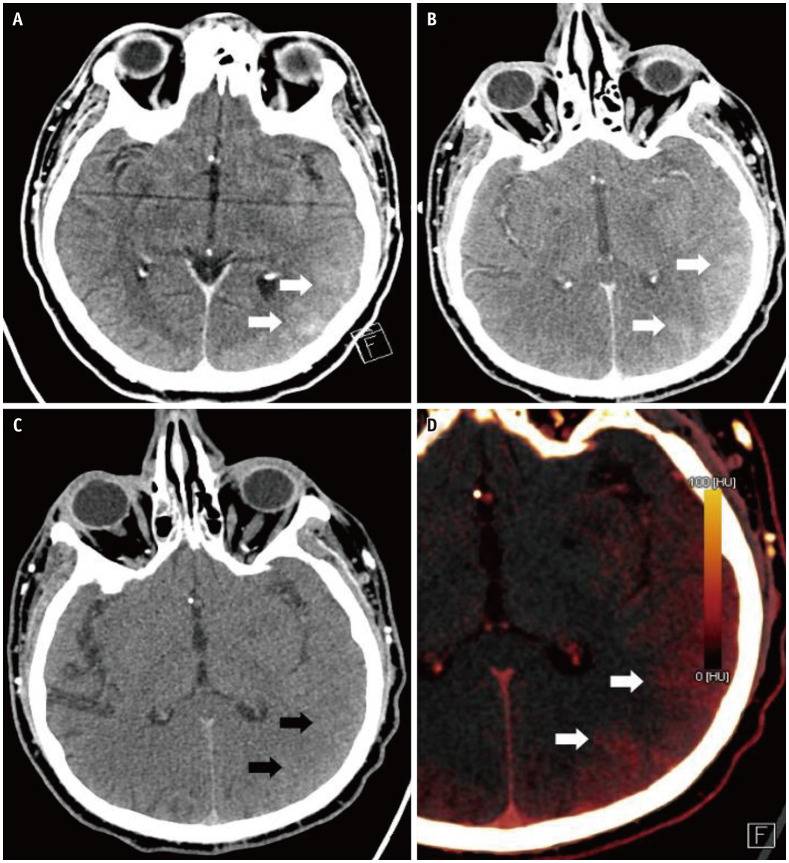
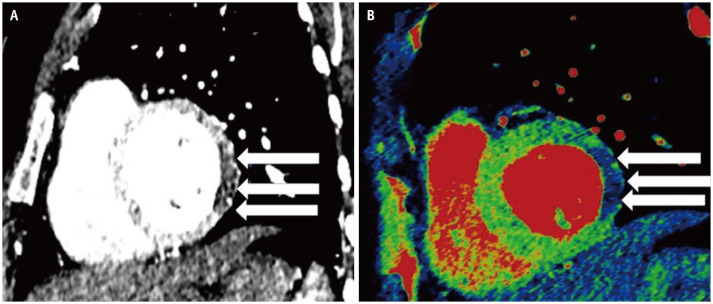
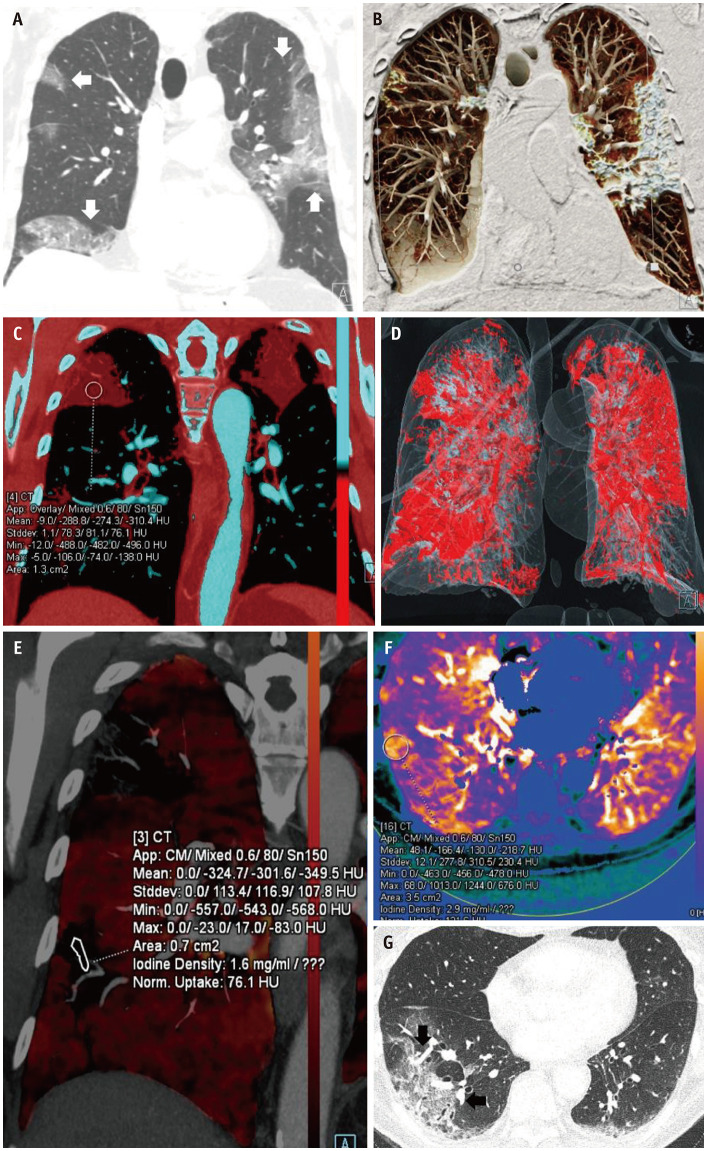
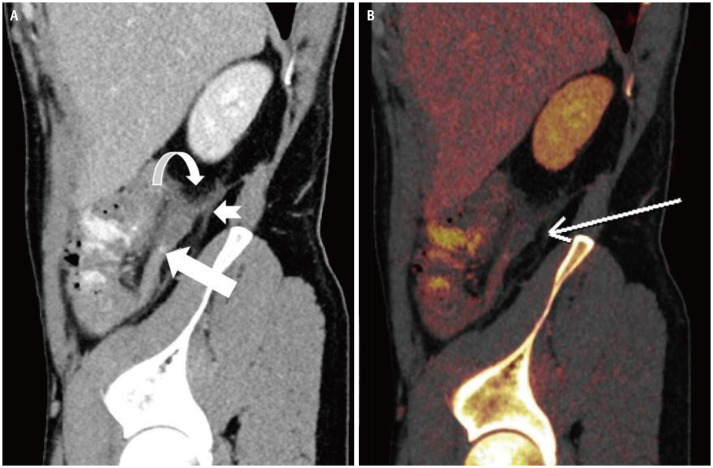
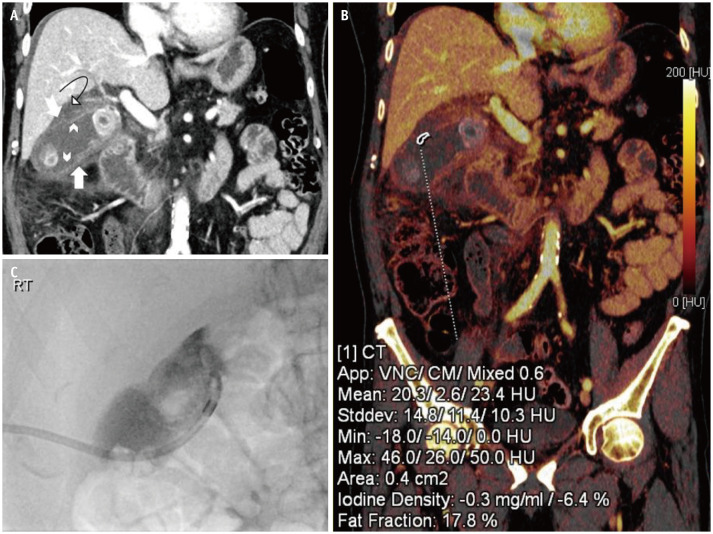
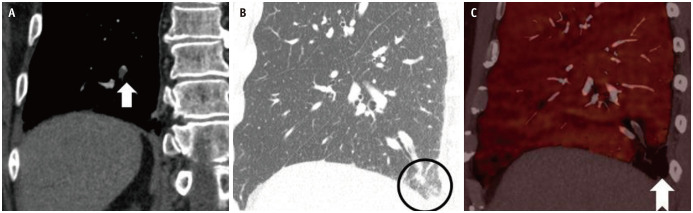
Dual-energy CT (DECT) provides insights into the material properties of tissues and can differentiate between tissues with similar attenuation on conventional single-energy imaging. In the conventional CT scanner, differences in the X-ray attenuation between adjacent structures are dependent on the atomic number of the materials involved, whereas in DECT, the difference in the attenuation is dependent on both the atomic number and electron density. The basic principle of DECT is to obtain two datasets with different X-ray energy levels from the same anatomic region and material decomposition based on attenuation differences at different energy levels. In this article, we discuss the clinical applications of DECT and its potential robust improvements in performance and postprocessing capabilities.
Keywords: Acute hemorrhage; COVID-19; DECT; Metal artifacts.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Grajo JR, Patino M, Prochowski A, Sahani DV. Dual energy CT in practice: basic principles and applications. Appl Radiol. 2016;45:6–12.
-
- Patel BN, Thomas JV, Lockhart ME, Berland LL, Morgan DE. Single-source dual-energy spectral multidetector CT of pancreatic adenocarcinoma: optimization of energy level viewing significantly increases lesion contrast. Clin Radiol. 2013;68:148–154. - PubMed
-
- Matsumoto K, Jinzaki M, Tanami Y, Ueno A, Yamada M, Kuribayashi S. Virtual monochromatic spectral imaging with fast kilovoltage switching: improved image quality as compared with that obtained with conventional 120-kVp CT. Radiology. 2011;259:257–262. - PubMed
-
- Wichmann JL, Nöske EM, Kraft J, Burck I, Wagenblast J, Eckardt A, et al. Virtual monoenergetic dual-energy computed tomography: optimization of kiloelectron volt settings in head and neck cancer. Invest Radiol. 2014;49:735–741. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
