

Norepinephrine in Septic Shock: A Systematic Review and Meta-analysis
- PMID: 33856300
- PMCID: PMC7972398
- DOI: 10.5811/westjem.2020.10.47825
Norepinephrine in Septic Shock: A Systematic Review and Meta-analysis
Abstract
Introduction: Most experts recommend norepinephrine as the first-line agent in septic shock. Our objective was to determine the effectiveness and safety of norepinephrine in patients with septic shock.
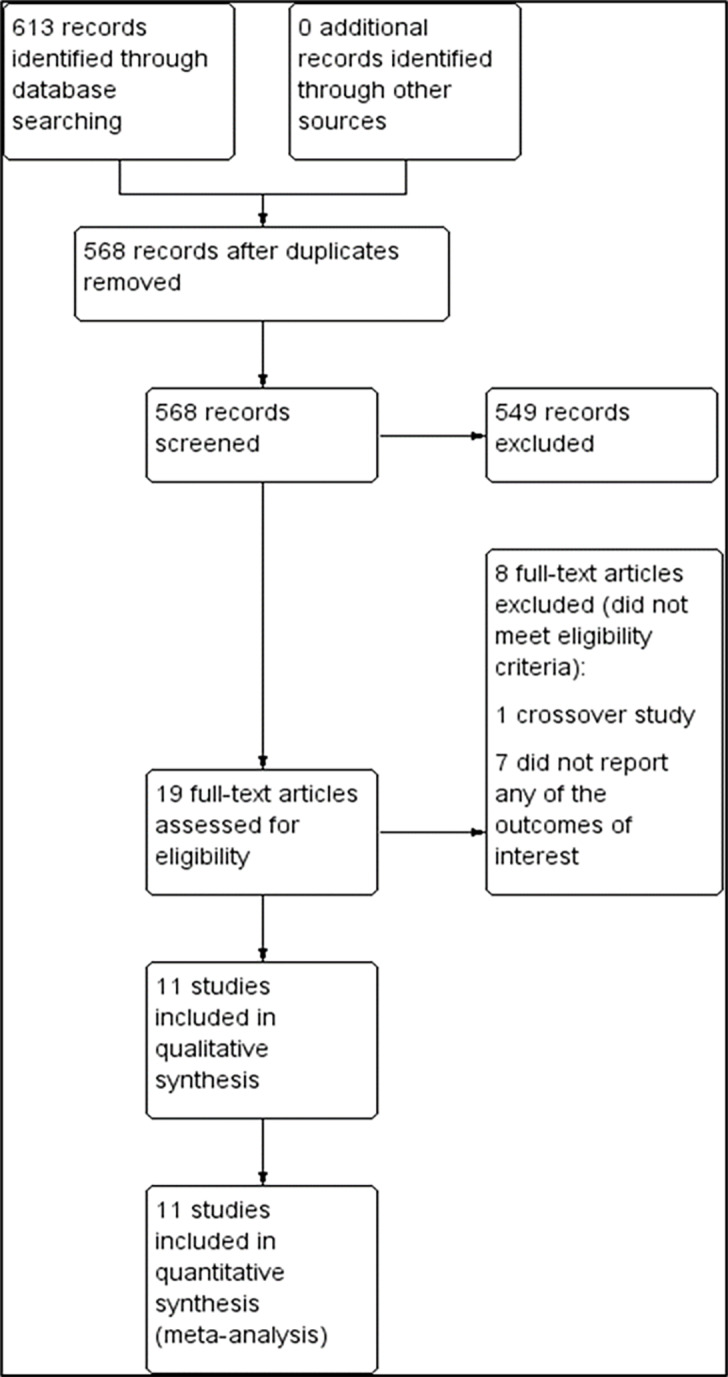
Methods: We searched the Cochrane Central Register of Controlled Trials and Epistemonikos, as well as MEDLINE from 1966 till August 2019. Screening of full texts, evaluation for eligibility, and data extraction were done by four independent reviewers. We estimated risk ratios (RR) and mean differences (MD) using a random-effects model with 95% confidence intervals (CI). The primary outcomes included the number of participants who achieved the target mean arterial pressure (MAP), time to achieve the target MAP, and number of participants with all-cause 28-day mortality. The secondary outcomes included the length of stay in the intensive care unit, length of hospital stay, incidence of arrhythmia and myocardial infarction, vasopressor-free days, and number of participants with all-cause 90-day mortality.
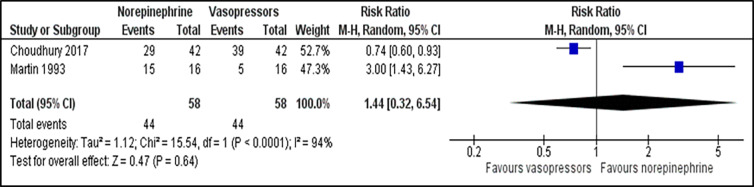
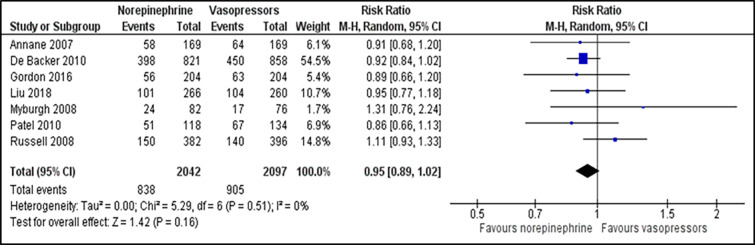
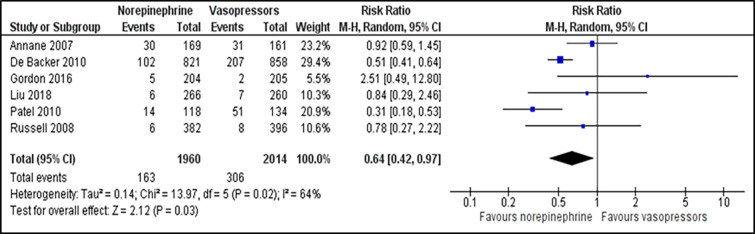
Results: We identified 11 randomized controlled trials with a total of 4,803 participants. There was no difference in the number of participants who achieved the target MAP between those patients receiving norepinephrine and other vasopressors (RR 1.44; 95% CI, 0.32 to 6.54; P = 0.640; I2 = 94%; two trials, 116 participants). There was no significant difference in time to achieve the target MAP (MD -0.05; 95%, CI, -0.32 to 0.21; P = 0.690; I2 = 26%; two trials, 1763 participants) and all-cause 28-day mortality (RR 0.95; 95% CI, 0.89 to 1.02; P = 0.160; I2 = 0%; seven trials, 4,139 participants). Regarding the secondary outcome, norepinephrine may significantly reduce the incidence of arrhythmia as compared to other vasopressors (RR 0.64; 95% CI, 0.42 to 0.97; P = 0.030; I2 = 64%; six trials, 3974 participants). There was no difference in the incidence of myocardial infarction (RR 1.28; 95% CI, 0.79 to 2.09), vasopressor-free day (RR 0.46; 95% CI, -1.82 to 2.74) and all-cause 90-day mortality (RR 1.08; 95% CI, 0.96 to 1.21) between norepinephrine and vasopressors.
Conclusion: In minimizing the occurrence of an arrhythmia, norepinephrine is superior to other vasopressors, making it safe to be used in septic shock. However, there was insufficient evidence concerning mortality and achievement of the target MAP outcomes.
Conflict of interest statement
Figures
References
-
- Keeley A, Hine P, Nsutebu E. The recognition and management of sepsis and septic shock: a guide for non-intensivists. Postgrad Med J. 2017;93(1104):626–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources