

Safety and Effectiveness of Weekly Carfilzomib, Lenalidomide, Dexamethasone, and Daratumumab Combination Therapy for Patients With Newly Diagnosed Multiple Myeloma: The MANHATTAN Nonrandomized Clinical Trial
- PMID: 33856405
- PMCID: PMC8050789
- DOI: 10.1001/jamaoncol.2021.0611
Safety and Effectiveness of Weekly Carfilzomib, Lenalidomide, Dexamethasone, and Daratumumab Combination Therapy for Patients With Newly Diagnosed Multiple Myeloma: The MANHATTAN Nonrandomized Clinical Trial
Abstract
Importance: Recently, the benefit of adding daratumumab to the proteasome inhibitor-based, 3-drug combination of bortezomib, lenalidomide, and dexamethasone for patients with newly diagnosed multiple myeloma who underwent high-dose melphalan chemotherapy and autologous hemopoietic cell transplant was assessed. Here, we examine the addition of daratumumab to the second-generation proteasome inhibitor-based, 3-drug combination of carfilzomib, lenalidomide, and dexamethasone.
Objective: To assess the safety and effectiveness of carfilzomib-lenalidomide-dexamethasone-daratumumab combination therapy for patients with newly diagnosed multiple myeloma, in the absence of high-dose melphalan chemotherapy and autologous hemopoietic cell transplant.
Design, setting, and participants: Clinical and correlative pilot study at the Memorial Sloan Kettering Cancer Center in New York, New York. Patients with newly diagnosed multiple myeloma were enrolled between October 1, 2018, and November 15, 2019. The median follow-up from start of treatment was 20.3 months (95% CI, 19.2-21.9 months).
Interventions: Eight 28-day cycles with intravenous carfilzomib, 20/56 mg/m2 (days 1, 8, and 15); oral lenalidomide, 25 mg, (days 1-21); dexamethasone, 40 mg weekly, orally or intravenously (cycles 1-4), and 20 mg after cycle 4; and intravenous daratumumab, 16 mg/kg (days 1, 8, 15, and 22 [cycles 1-2]; days 1 and 15 [cycles 3-6]; and day 1 [cycles 7 and 8]).
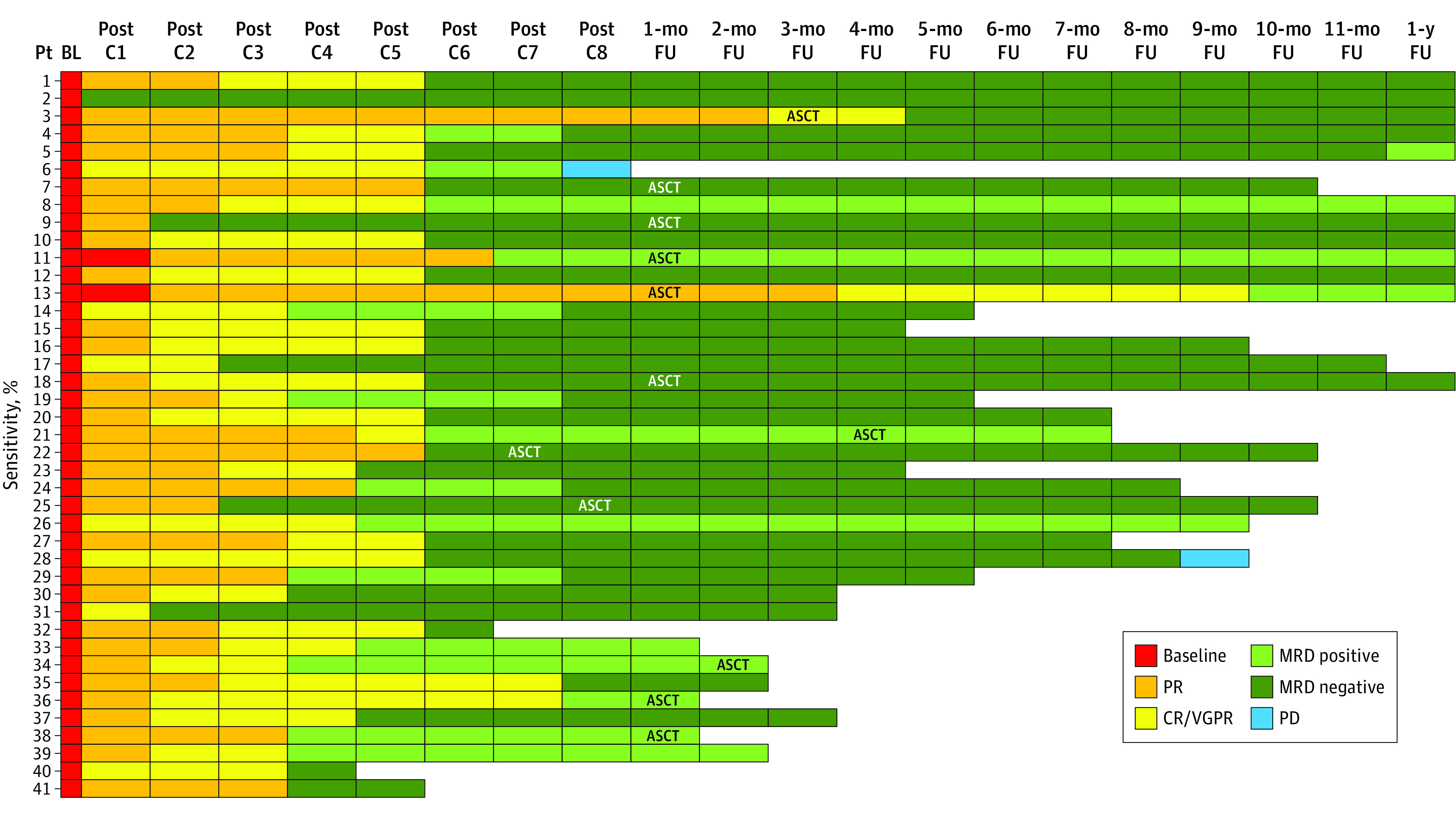
Main outcomes and measures: The primary end point was the minimal residual disease (MRD) rate, in the absence of high-dose melphalan chemotherapy and autologous hemopoietic cell transplant. Secondary end points included determining safety and tolerability, evaluating rates of clinical response per the International Myeloma Working Group, and estimating progression-free survival (PFS) and overall survival (OS) rates.
Results: Forty-one evaluable patients were enrolled (median age, 59 years; range, 30-70 years); 25 (61%) were female, and 20 (49%) had high-risk multiple myeloma. The primary end point (MRD negativity in the bone marrow; 10-5 sensitivity) was achieved in 29 of 41 patients (71%; 95% CI, 54%-83%), and therefore the trial was deemed successful. Median time to MRD negativity was 6 cycles (range, 1-8 cycles). Secondary end points of the overall response rate and the very good partial response or complete response rate were 100% (41 of 41 patients) and 95% (39 of 41 patients), respectively. At 11 months of the median follow-up, the 1-year PFS rate and the OS rate were 98% (95% CI, 93%-100%) and 100%, respectively. Most common (≥2 patients) grade 3 or 4 adverse events were neutropenia (12 patients [27%]), rash (4 patients [9%]), lung infection (3 patients [7%]), and increased alanine aminotransferase level (2 patients [4%]). There were no deaths.
Conclusions and relevance: In this nonrandomized clinical trial, carfilzomib-lenalidomide-dexamethasone-daratumumab combination therapy was associated with high rates of MRD negativity in patients with newly diagnosed multiple myeloma and high rates of PFS.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
