

Percutaneous Peripheral Nerve Stimulation (Neuromodulation) for Postoperative Pain: A Randomized, Sham-controlled Pilot Study
- PMID: 33856424
- PMCID: PMC8249357
- DOI: 10.1097/ALN.0000000000003776
Percutaneous Peripheral Nerve Stimulation (Neuromodulation) for Postoperative Pain: A Randomized, Sham-controlled Pilot Study
Abstract
Background: Percutaneous peripheral nerve stimulation is an analgesic technique involving the percutaneous implantation of a lead followed by the delivery of electric current using an external pulse generator. Percutaneous peripheral nerve stimulation has been used extensively for chronic pain, but only uncontrolled series have been published for acute postoperative pain. The current multicenter study was undertaken to (1) determine the feasibility and optimize the protocol for a subsequent clinical trial and (2) estimate the treatment effect of percutaneous peripheral nerve stimulation on postoperative pain and opioid consumption.
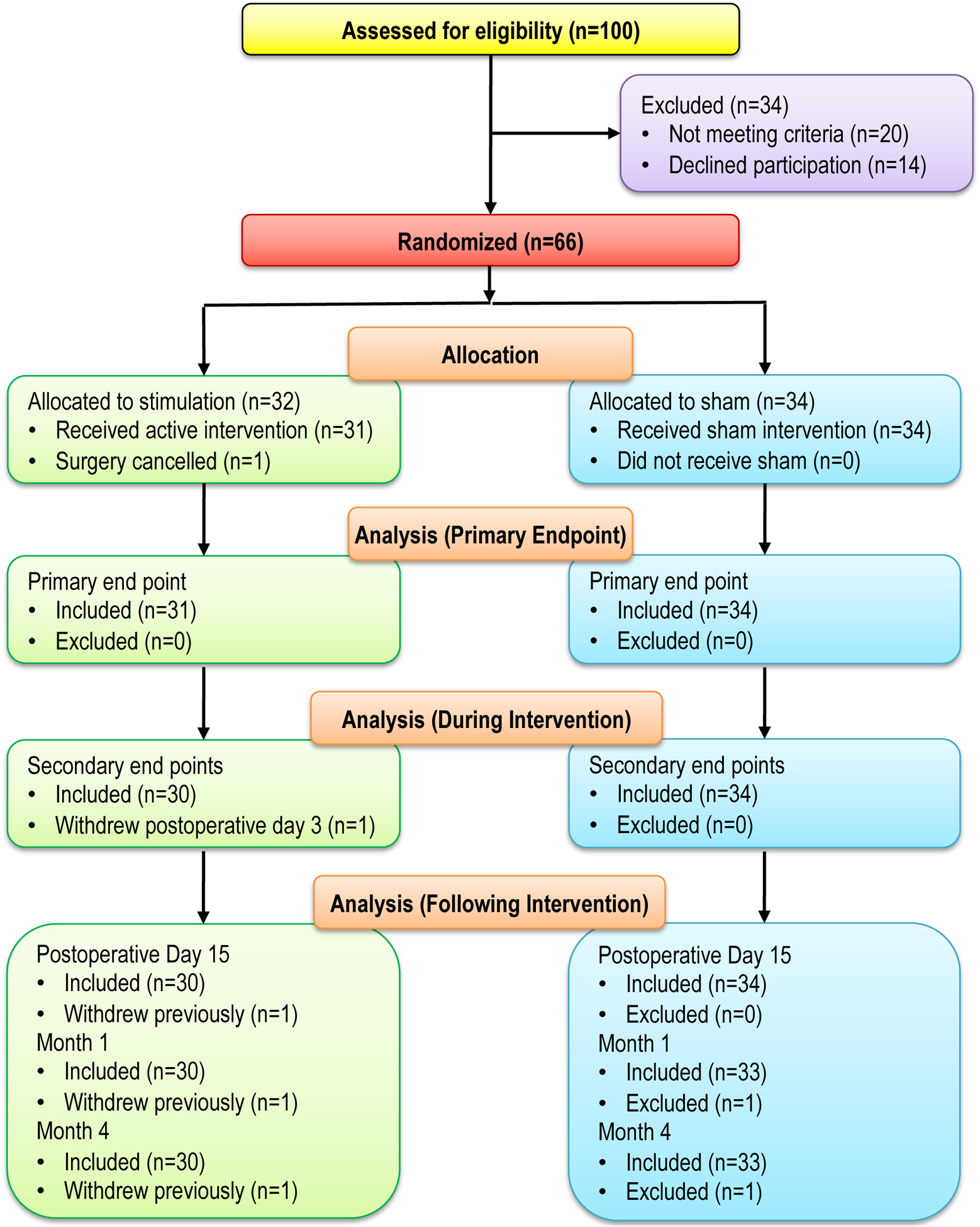
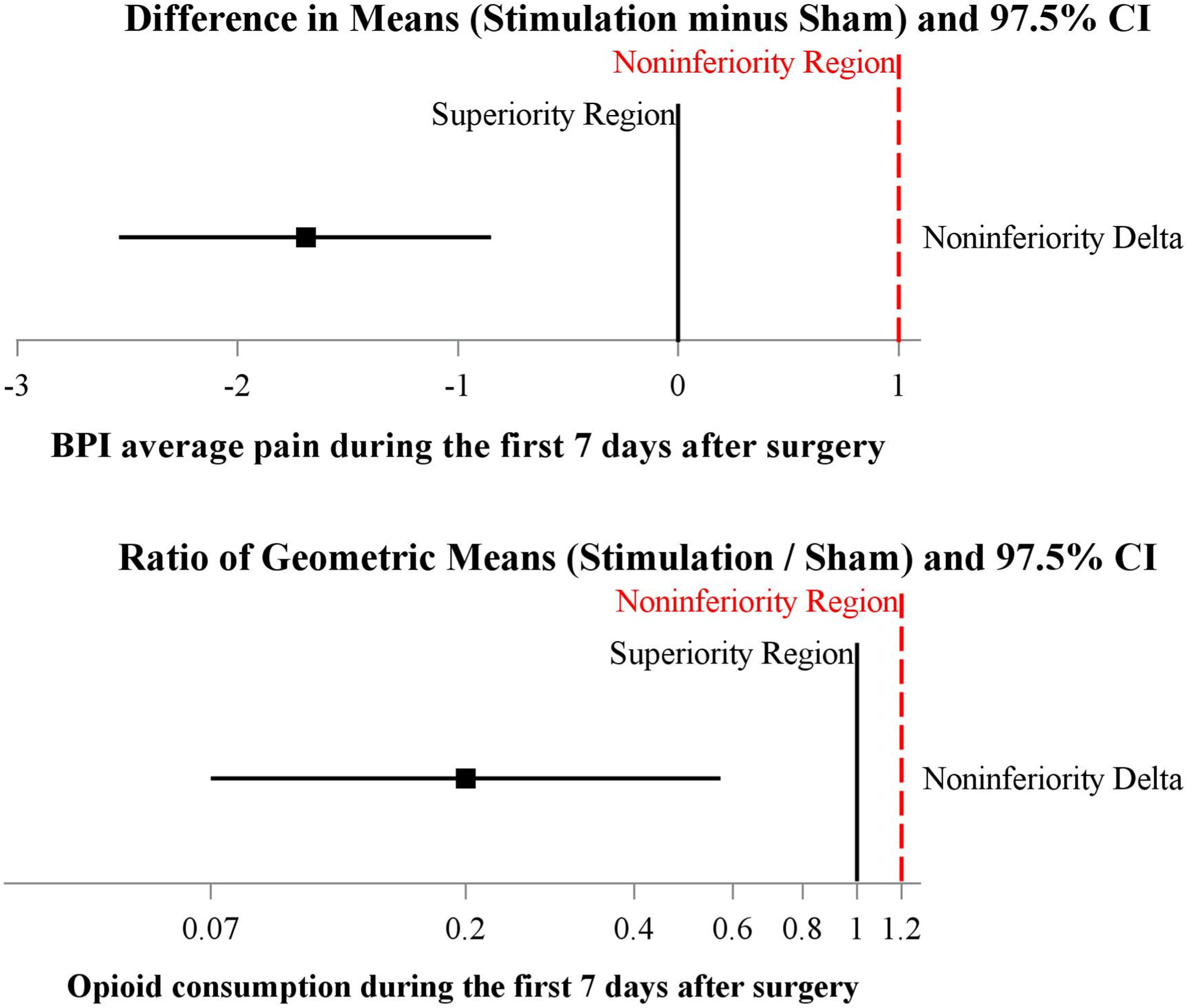
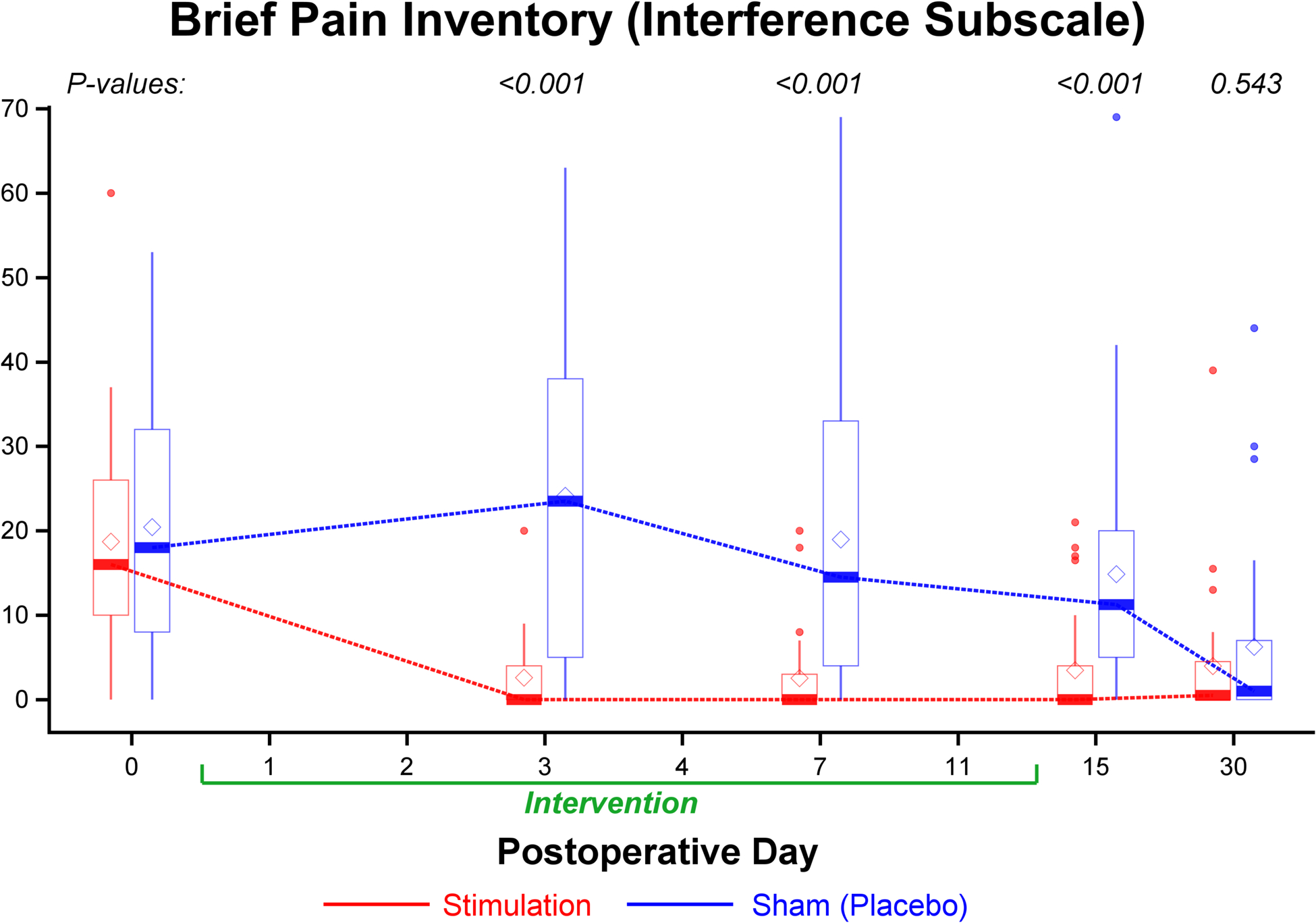
Methods: Preoperatively, an electrical lead was percutaneously implanted to target the sciatic nerve for major foot/ankle surgery (e.g., hallux valgus correction), the femoral nerve for anterior cruciate ligament reconstruction, or the brachial plexus for rotator cuff repair, followed by a single injection of long-acting local anesthetic along the same nerve/plexus. Postoperatively, participants were randomized to 14 days of either electrical stimulation (n = 32) or sham stimulation (n = 34) using an external pulse generator in a double-masked fashion. The dual primary treatment effect outcome measures were (1) cumulative opioid consumption (in oral morphine equivalents) and (2) mean values of the "average" daily pain scores measured on the 0 to 10 Numeric Rating Scale within the first 7 postoperative days.
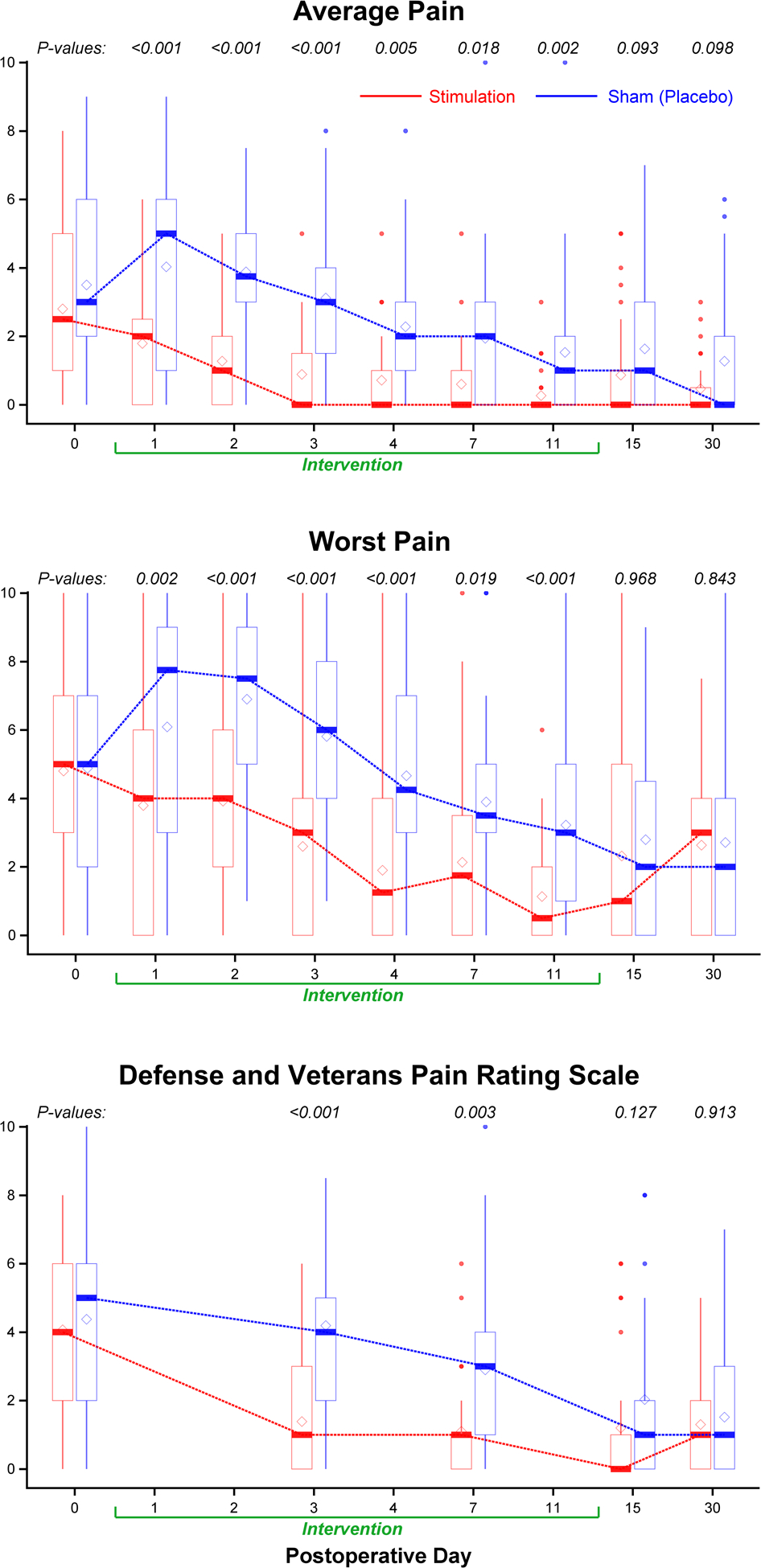
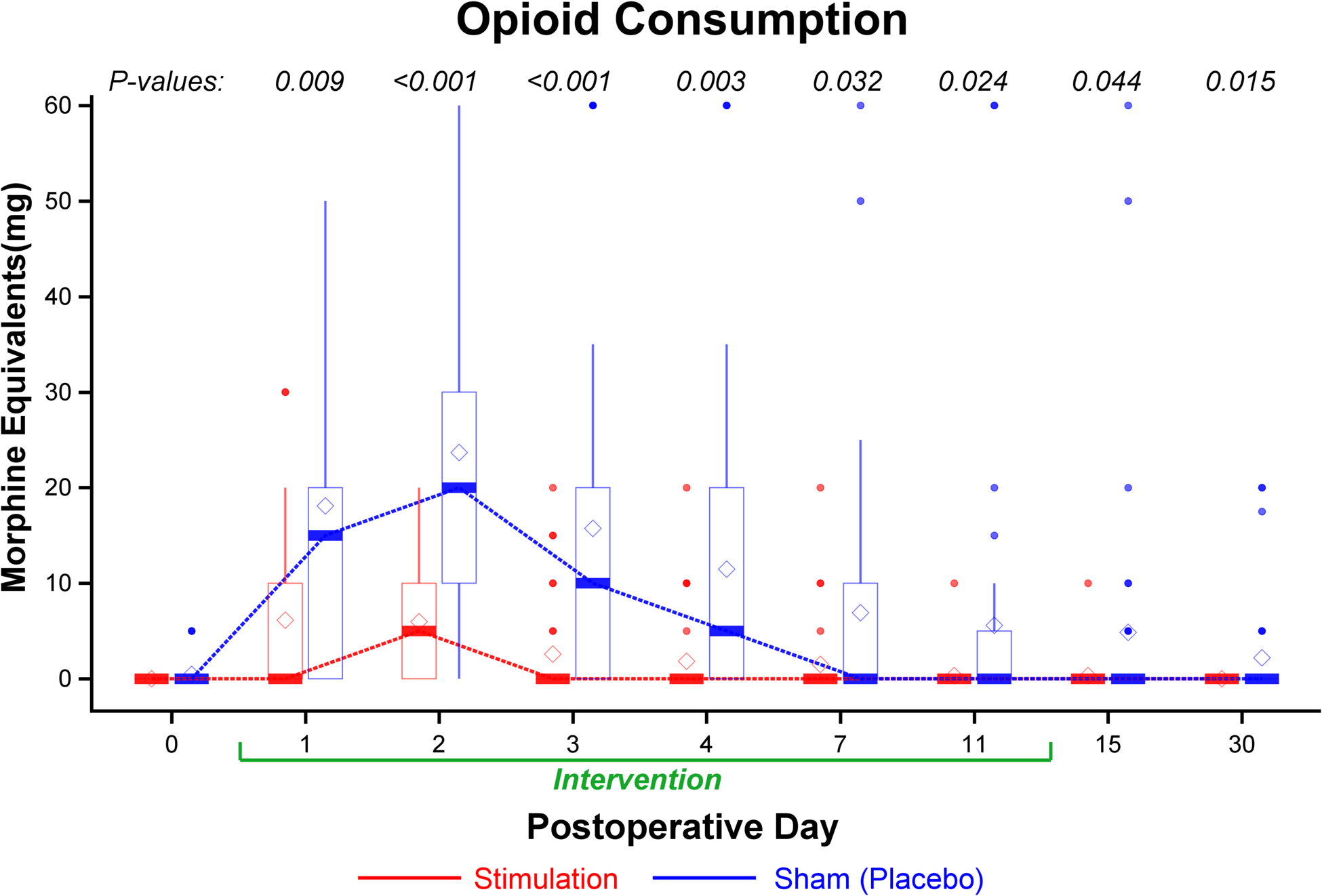
Results: During the first 7 postoperative days, opioid consumption in participants given active stimulation was a median (interquartile range) of 5 mg (0 to 30) versus 48 mg (25 to 90) in patients given sham treatment (ratio of geometric means, 0.20 [97.5% CI, 0.07 to 0.57]; P < 0.001). During this same period, the average pain intensity in patients given active stimulation was a mean ± SD of 1.1 ± 1.1 versus 3.1 ± 1.7 in those given sham (difference, -1.8 [97.5% CI, -2.6 to -0.9]; P < 0.001).
Conclusions: Percutaneous peripheral nerve stimulation reduced pain scores and opioid requirements free of systemic side effects during at least the initial week after ambulatory orthopedic surgery.
Copyright © 2021, the American Society of Anesthesiologists. All Rights Reserved.
Figures
References
-
- Cullen KA, Hall MJ, Golosinskiy A: Ambulatory surgery in the United States, 2006. National Health Statistics Reports; 2009: 1–25 - PubMed
-
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ: Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003; 97: 534–40 - PubMed
-
- Ilfeld BM, Vandenborne K, Duncan PW, Sessler DI, Enneking FK, Shuster JJ, Theriaque DW, Chmielewski TL, Spadoni EH, Wright TW: Ambulatory continuous interscalene nerve blocks decrease the time to discharge readiness after total shoulder arthroplasty: A randomized, triple-masked, placebo-controlled study. Anesthesiology 2006; 105: 999–1007 - PubMed
-
- Kehlet H, Jensen TS, Woolf CJ: Persistent postsurgical pain: risk factors and prevention. Lancet 2006; 367: 1618–25 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
