

Association of Race/Ethnicity, Gender, and Socioeconomic Status With Sodium-Glucose Cotransporter 2 Inhibitor Use Among Patients With Diabetes in the US
- PMID: 33856475
- PMCID: PMC8050743
- DOI: 10.1001/jamanetworkopen.2021.6139
Association of Race/Ethnicity, Gender, and Socioeconomic Status With Sodium-Glucose Cotransporter 2 Inhibitor Use Among Patients With Diabetes in the US
Abstract
Importance: Sodium-glucose cotransporter 2 (SGLT2) inhibitors significantly reduce deaths from cardiovascular conditions, hospitalizations for heart failure, and progression of kidney disease among patients with type 2 diabetes. Black individuals have a disproportionate burden of cardiovascular and chronic kidney disease (CKD). Adoption of novel therapeutics has been slower among Black and female patients and among patients with low socioeconomic status than among White or male patients or patients with higher socioeconomic status.
Objective: To assess whether inequities based on race/ethnicity, gender, and socioeconomic status exist in SGLT2 inhibitor use among patients with type 2 diabetes in the US.
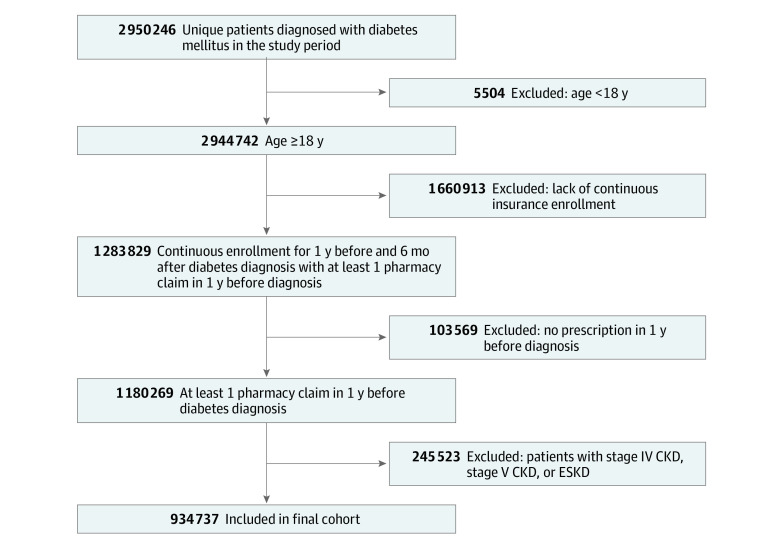
Design, setting, and participants: This retrospective cohort study of commercially insured patients in the US was performed from October 1, 2015, to June 30, 2019, using the Optum Clinformatics Data Mart. Adult patients with a diagnosis of type 2 diabetes, including those with heart failure with reduced ejection fraction (HFrEF), atherosclerotic cardiovascular disease (ASCVD), or CKD, were evaluated in the analysis.
Main outcomes and measures: Prescription of an SGLT2 inhibitor. Multivariable logistic regression models were used to assess the association of race/ethnicity, gender, and socioeconomic status with SGLT2 inhibitor use.
Results: Of 934 737 patients with type 2 diabetes (mean [SD] age, 65.4 [12.9] years; 50.7% female; 57.6% White), 81 007 (8.7%) were treated with an SGLT2 inhibitor during the study period. Between 2015 and 2019, the percentage of patients with type 2 diabetes treated with an SGLT2 inhibitor increased from 3.8% to 11.9%. Among patients with type 2 diabetes and cardiovascular or kidney disease, the rate of SGLT2 inhibitor use increased but was lower than that among all patients with type 2 diabetes (HFrEF: 1.9% to 7.6%; ASCVD: 3.0% to 9.8%; CKD: 2.1% to 7.5%). In multivariable analyses, Black race (adjusted odds ratio [aOR], 0.83; 95% CI, 0.81-0.85), Asian race (aOR, 0.94; 95% CI, 0.90-0.98), and female gender (aOR, 0.84; 95% CI, 0.82-0.85) were associated with lower rates of SGLT2 inhibitor use, whereas higher median household income (≥$100 000: aOR, 1.08 [95% CI, 1.05-1.10]; $50 000-$99 999: aOR, 1.05 [95% CI, 1.03-1.07] vs <$50 000) was associated with a higher rate of SGLT2 inhibitor use. These results were similar among patients with HFrEF, ASCVD, and CKD.
Conclusions and relevance: In this cohort study, use of an SGLT2 inhibitor treatment increased among patients with type 2 diabetes from 2015 to 2019 but remained low, particularly among patients with HFrEF, CKD, and ASCVD. Black and female patients and patients with low socioeconomic status were less likely to receive an SGLT2 inhibitor, suggesting that interventions to ensure more equitable use are essential to prevent worsening of well-documented disparities in cardiovascular and kidney outcomes in the US.
Conflict of interest statement
Figures


References
-
- Sarwar N, Gao P, Seshasai SR, et al. ; Emerging Risk Factors Collaboration . Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215-2222. doi: 10.1016/S0140-6736(10)60484-9 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
