

The influence of digital PET/CT on diagnostic certainty and interrater reliability in [68Ga]Ga-PSMA-11 PET/CT for recurrent prostate cancer
- PMID: 33856522
- PMCID: PMC8452558
- DOI: 10.1007/s00330-021-07870-5
The influence of digital PET/CT on diagnostic certainty and interrater reliability in [68Ga]Ga-PSMA-11 PET/CT for recurrent prostate cancer
Abstract
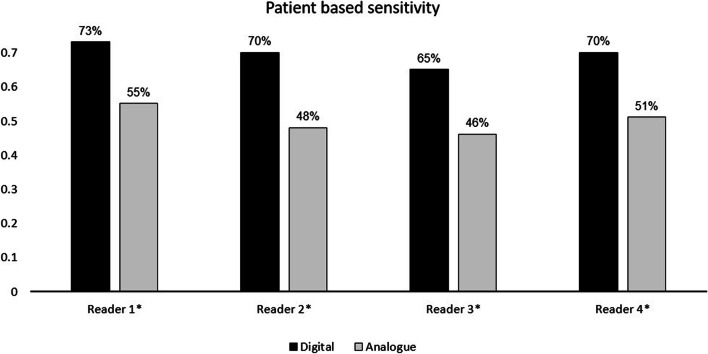
Objective: To investigate the impact of digital PET/CT on diagnostic certainty, patient-based sensitivity and interrater reliability.
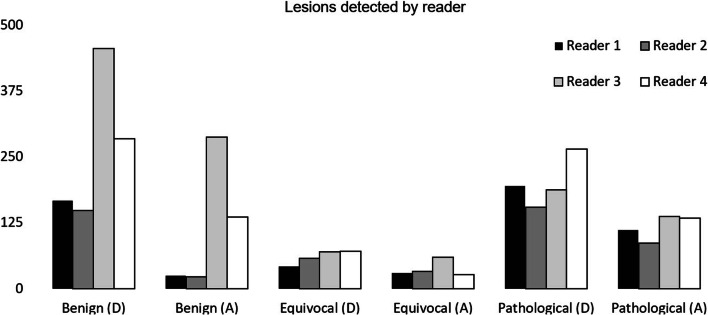
Methods: Four physicians retrospectively evaluated two matched cohorts of patients undergoing [68Ga]Ga-PSMA-11 PET/CT on a digital (dPET/CT n = 65) or an analogue scanner (aPET/CT n = 65) for recurrent prostate cancer between 11/2018 and 03/2019. The number of equivocal and pathological lesions as well as the frequency of discrepant findings and the interrater reliability for the two scanners were compared.
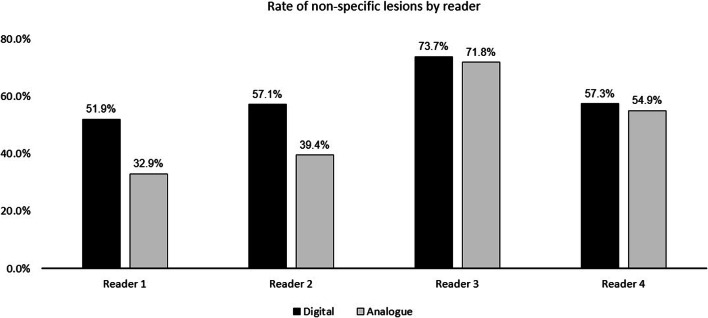
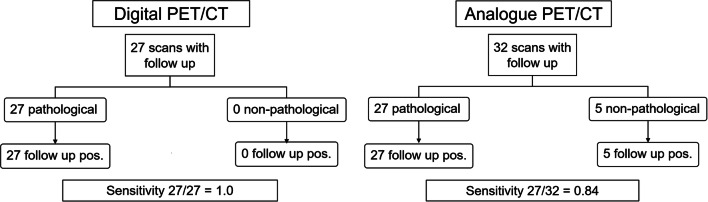
Results: dPET/CT detected more lesions than aPET/CT (p < 0.001). A higher number of pathological scans were observed for dPET/CT (83% vs. 57%, p < 0.001). The true-positive rate at follow-up was 100% for dPET/CT compared to 84% for aPET/CT (p < 0.001). The proportion of lesions rated as non-pathological as a total of all PSMA-avid lesions detected for dPET/CT was comparable to aPET/CT (61.8% vs. 57.0%, p = 0.99). Neither a higher rate of diagnostically uncertain lesions (11.5% dPET/CT vs. 13.7% aPET/CT, p = 0.95) nor discrepant scans (where one or more readers differed in opinion as to whether the scan is pathological) were observed (18% dPET/CT vs. 17% aPET/CT, p = 0.76). Interrater reliability for pathological lesions was excellent for both scanner types (Cronbach's α = 0.923 dPET/CT; α = 0.948 aPET/CT) and interrater agreement was substantial for dPET/CT (Krippendorf's α = 0.701) and almost perfect in aPET/CT (α = 0.802).
Conclusions: A higher detection rate for pathological lesions for dPET/CT compared with aPET/CT in multiple readers was observed. This improved sensitivity was coupled with an improved true-positive rate and was not associated with increased diagnostic uncertainty, rate of non-specific lesions, or reduced interrater reliability.
Key points: • New generation digital scanners detect more cancer lesions in men with prostate cancer. • When using digital scanners, the doctors are able to diagnose prostate cancer lesions with better certainty • When using digital scanners, the doctors do not disagree with each other more than with other scanner types.
Keywords: Molecular imaging; Nuclear medicine; Positron emission tomography; Prostate cancer.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

Similar articles
-
Digital versus analogue PET in [68Ga]Ga-PSMA-11 PET/CT for recurrent prostate cancer: a matched-pair comparison.Eur J Nucl Med Mol Imaging. 2020 Mar;47(3):614-623. doi: 10.1007/s00259-019-04630-y. Epub 2019 Dec 2. Eur J Nucl Med Mol Imaging. 2020. PMID: 31792572
-
Comparison of Digital versus Analog 68Ga-PSMA-11 PET/CT Performance in Hormone-Sensitive Prostate Cancer Patients with Early Biochemical Recurrence or Persistence after Radical Treatment.Diagnostics (Basel). 2023 Nov 26;13(23):3535. doi: 10.3390/diagnostics13233535. Diagnostics (Basel). 2023. PMID: 38066776 Free PMC article.
-
Digital PET and detection of recurrent prostate cancer: what have we gained, and what is still missing?Expert Rev Med Devices. 2021 Nov;18(11):1107-1110. doi: 10.1080/17434440.2021.1990036. Epub 2021 Oct 13. Expert Rev Med Devices. 2021. PMID: 34608848
-
68Ga-Labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-analysis.Eur Urol Focus. 2018 Sep;4(5):686-693. doi: 10.1016/j.euf.2016.11.002. Epub 2016 Nov 15. Eur Urol Focus. 2018. PMID: 28753806
-
68Ga-PSMA-PET/CT Has a Role in Detecting Prostate Cancer Lesions in Patients with Recurrent Disease.Anticancer Res. 2017 Jun;37(6):2753-2760. doi: 10.21873/anticanres.11627. Anticancer Res. 2017. PMID: 28551611 Review.
Cited by
-
Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study.Biomedicines. 2022 Jan 15;10(1):177. doi: 10.3390/biomedicines10010177. Biomedicines. 2022. PMID: 35052856 Free PMC article.
-
Comparison of digital and analog [68Ga]Ga-PSMA-11 PET/CT for detecting post-prostatectomy biochemical recurrence in prostate cancer patients: a prospective study.Sci Rep. 2024 Jul 1;14(1):14989. doi: 10.1038/s41598-024-65399-1. Sci Rep. 2024. PMID: 38951530 Free PMC article.
-
The clinical acceptability of short versus long duration acquisitions for head and neck cancer using long-axial field-of-view PET/CT: a retrospective evaluation.Eur J Nucl Med Mol Imaging. 2024 Apr;51(5):1436-1443. doi: 10.1007/s00259-023-06516-6. Epub 2023 Dec 14. Eur J Nucl Med Mol Imaging. 2024. PMID: 38095670 Free PMC article.
-
Long-axial field-of-view PET/CT: perspectives and review of a revolutionary development in nuclear medicine based on clinical experience in over 7000 patients.Cancer Imaging. 2023 Mar 18;23(1):28. doi: 10.1186/s40644-023-00540-3. Cancer Imaging. 2023. PMID: 36934273 Free PMC article. Review.
-
Assessment of malignancy and PSMA expression of uncertain bone foci in [18F]PSMA-1007 PET/CT for prostate cancer-a single-centre experience of PET-guided biopsies.Eur J Nucl Med Mol Imaging. 2022 Sep;49(11):3910-3916. doi: 10.1007/s00259-022-05745-5. Epub 2022 Apr 28. Eur J Nucl Med Mol Imaging. 2022. PMID: 35482114 Free PMC article.
References
-
- Schillaci O, Urbano N (2019) Digital PET/CT: a new intriguing chance for clinical nuclear medicine and personalized molecular imaging. Eur J Nucl Med Mol Imaging. 10.1007/s00259-019-04300-z - PubMed
-
- van Sluis JJ, de Jong J, Schaar J et al (2019) Performance characteristics of the digital Biograph Vision PET/CT system. J Nucl Med. 10.2967/jnumed.118.215418 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
