

Diagnostic performance of artificial intelligence model for pneumonia from chest radiography
- PMID: 33857181
- PMCID: PMC8049482
- DOI: 10.1371/journal.pone.0249399
Diagnostic performance of artificial intelligence model for pneumonia from chest radiography
Abstract
Objective: The chest X-ray (CXR) is the most readily available and common imaging modality for the assessment of pneumonia. However, detecting pneumonia from chest radiography is a challenging task, even for experienced radiologists. An artificial intelligence (AI) model might help to diagnose pneumonia from CXR more quickly and accurately. We aim to develop an AI model for pneumonia from CXR images and to evaluate diagnostic performance with external dataset.
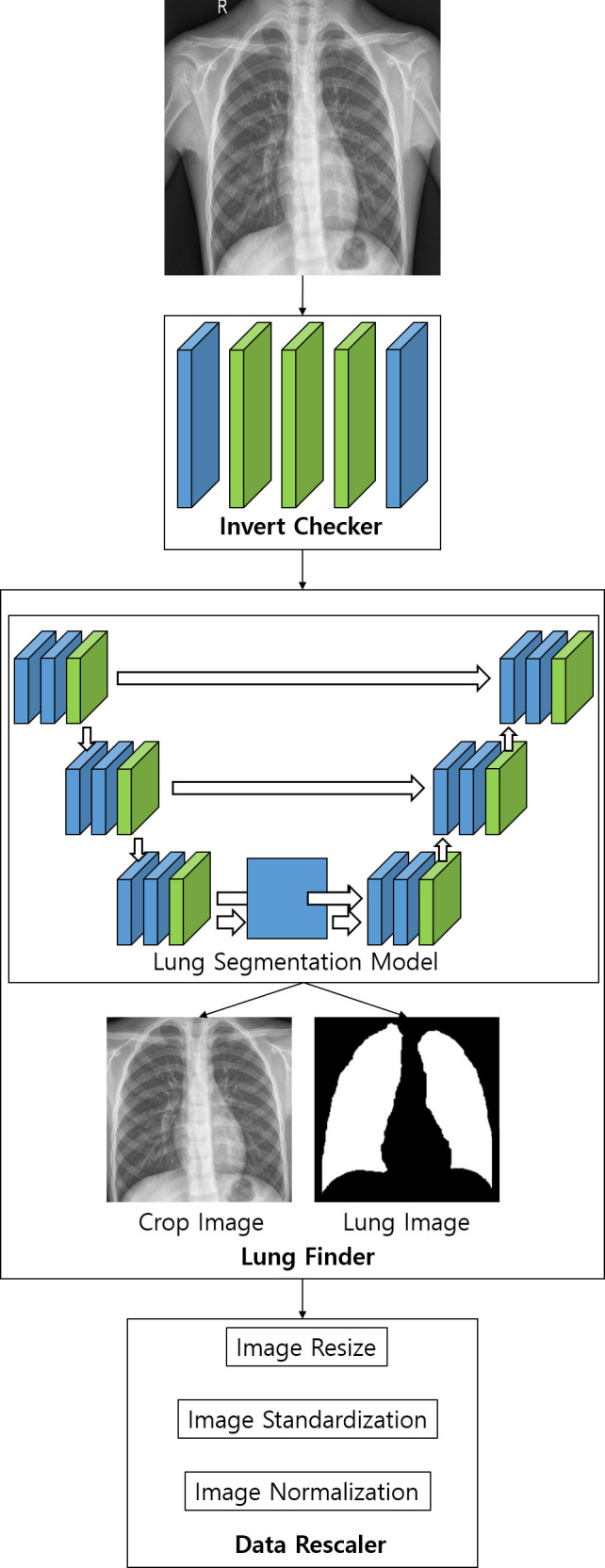
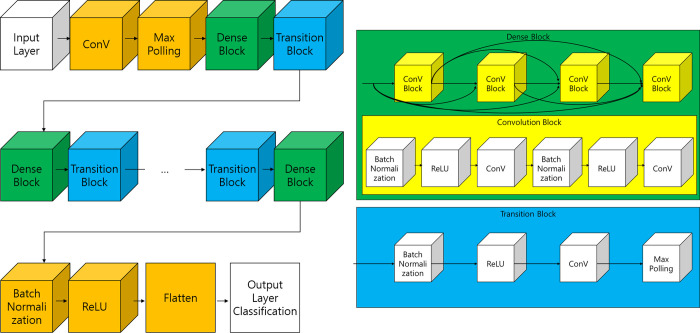
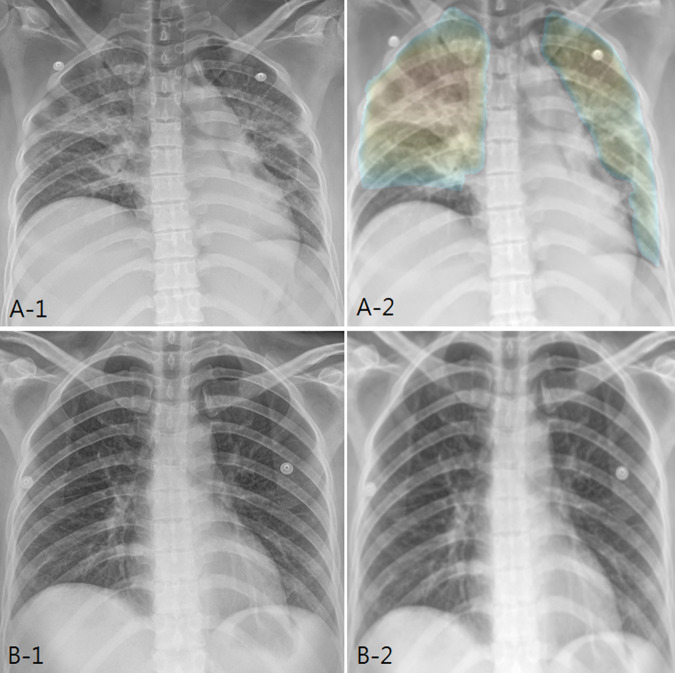
Methods: To train the pneumonia model, a total of 157,016 CXR images from the National Institutes of Health (NIH) and the Korean National Tuberculosis Association (KNTA) were used (normal vs. pneumonia = 120,722 vs.36,294). An ensemble model of two neural networks with DenseNet classifies each CXR image into pneumonia or not. To test the accuracy of the models, a separate external dataset of pneumonia CXR images (n = 212) from a tertiary university hospital (Gachon University Gil Medical Center GUGMC, Incheon, South Korea) was used; the diagnosis of pneumonia was based on both the chest CT findings and clinical information, and the performance evaluated using the area under the receiver operating characteristic curve (AUC). Moreover, we tested the change of the AI probability score for pneumonia using the follow-up CXR images (7 days after the diagnosis of pneumonia, n = 100).
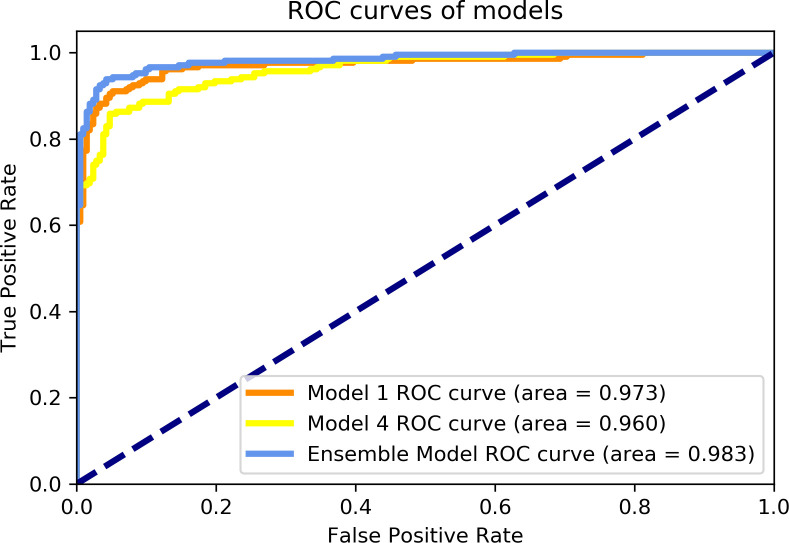
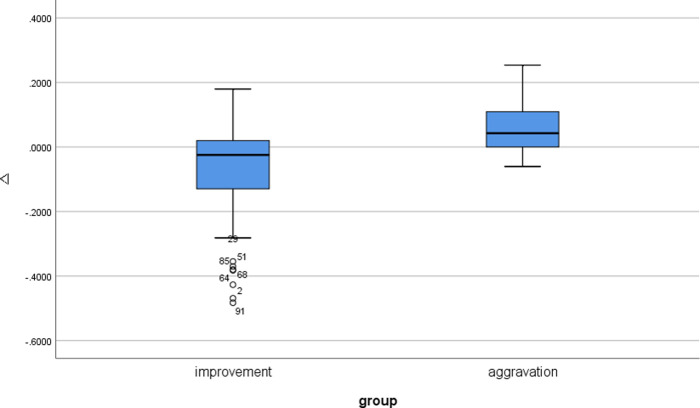
Results: When the probability scores of the models that have a threshold of 0.5 for pneumonia, two models (models 1 and 4) having different pre-processing parameters on the histogram equalization distribution showed best AUC performances of 0.973 and 0.960, respectively. As expected, the ensemble model of these two models performed better than each of the classification models with 0.983 AUC. Furthermore, the AI probability score change for pneumonia showed a significant difference between improved cases and aggravated cases (Δ = -0.06 ± 0.14 vs. 0.06 ± 0.09, for 85 improved cases and 15 aggravated cases, respectively, P = 0.001) for CXR taken as a 7-day follow-up.
Conclusions: The ensemble model combined two different classification models for pneumonia that performed at 0.983 AUC for an external test dataset from a completely different data source. Furthermore, AI probability scores showed significant changes between cases of different clinical prognosis, which suggest the possibility of increased efficiency and performance of the CXR reading at the diagnosis and follow-up evaluation for pneumonia.
Conflict of interest statement
The authors have read the journal’s policy and the authors of this manuscript have the following competing interests: TK, DK, ML, and SUK are paid employees of JLK Inc. and JJ was a paid employee of JLK Inc. at the time of study. KGK received a research grant from JLK Inc. for activities not related to the present article. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no patents, products in development or marketed products associated with this research to declare.
Figures
Similar articles
-
Thorax computed tomography (CTX) guided ground truth annotation of CHEST radiographs (CXR) for improved classification and detection of COVID-19.Int J Numer Method Biomed Eng. 2024 Jun;40(6):e3823. doi: 10.1002/cnm.3823. Epub 2024 Apr 8. Int J Numer Method Biomed Eng. 2024. PMID: 38587026
-
AI-based computer-aided diagnostic system of chest digital tomography synthesis: Demonstrating comparative advantage with X-ray-based AI systems.Comput Methods Programs Biomed. 2023 Oct;240:107643. doi: 10.1016/j.cmpb.2023.107643. Epub 2023 Jun 5. Comput Methods Programs Biomed. 2023. PMID: 37348439
-
Multi-View Ensemble Convolutional Neural Network to Improve Classification of Pneumonia in Low Contrast Chest X-Ray Images.Annu Int Conf IEEE Eng Med Biol Soc. 2020 Jul;2020:1238-1241. doi: 10.1109/EMBC44109.2020.9176517. Annu Int Conf IEEE Eng Med Biol Soc. 2020. PMID: 33018211
-
Artificial Intelligence and COVID-19 Using Chest CT Scan and Chest X-ray Images: Machine Learning and Deep Learning Approaches for Diagnosis and Treatment.J Pers Med. 2021 Sep 30;11(10):993. doi: 10.3390/jpm11100993. J Pers Med. 2021. PMID: 34683133 Free PMC article. Review.
-
Accuracy of deep learning for automated detection of pneumonia using chest X-Ray images: A systematic review and meta-analysis.Comput Biol Med. 2020 Aug;123:103898. doi: 10.1016/j.compbiomed.2020.103898. Epub 2020 Jul 14. Comput Biol Med. 2020. PMID: 32768045
Cited by
-
AI for Detection of Tuberculosis: Implications for Global Health.Radiol Artif Intell. 2024 Mar;6(2):e230327. doi: 10.1148/ryai.230327. Radiol Artif Intell. 2024. PMID: 38197795 Free PMC article.
-
Incidentally found resectable lung cancer with the usage of artificial intelligence on chest radiographs.PLoS One. 2023 Mar 10;18(3):e0281690. doi: 10.1371/journal.pone.0281690. eCollection 2023. PLoS One. 2023. PMID: 36897865 Free PMC article.
-
Deep Learning in Multi-Class Lung Diseases' Classification on Chest X-ray Images.Diagnostics (Basel). 2022 Apr 6;12(4):915. doi: 10.3390/diagnostics12040915. Diagnostics (Basel). 2022. PMID: 35453963 Free PMC article.
-
Incidence and Outcomes of Non-Ventilator-Associated Hospital-Acquired Pneumonia in 284 US Hospitals Using Electronic Surveillance Criteria.JAMA Netw Open. 2023 May 1;6(5):e2314185. doi: 10.1001/jamanetworkopen.2023.14185. JAMA Netw Open. 2023. PMID: 37200031 Free PMC article.
-
Chest X-ray in Emergency Radiology: What Artificial Intelligence Applications Are Available?Diagnostics (Basel). 2023 Jan 6;13(2):216. doi: 10.3390/diagnostics13020216. Diagnostics (Basel). 2023. PMID: 36673027 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
