

Repeated intermittent hypoxic stimuli to operative lung reduce hypoxemia during subsequent one-lung ventilation for thoracoscopic surgery: A randomized controlled trial
- PMID: 33857201
- PMCID: PMC8049270
- DOI: 10.1371/journal.pone.0249880
Repeated intermittent hypoxic stimuli to operative lung reduce hypoxemia during subsequent one-lung ventilation for thoracoscopic surgery: A randomized controlled trial
Abstract
Background: An intervention to potentiate hypoxic pulmonary vasoconstriction may reduce intrapulmonary shunt and hypoxemia during one-lung ventilation. Previous animal studies reported that repeated intermittent hypoxic stimuli potentiated hypoxic pulmonary vasoconstriction, but no clinical study has examined the effects of this intervention on hypoxemia during one-lung ventilation. We thus performed a single-center, parallel-group, double-blind, randomized controlled trial to investigate whether repeated intermittent hypoxic stimuli to the operative lung reduce hypoxemia during the subsequent one-lung ventilation for thoracoscopic surgery.
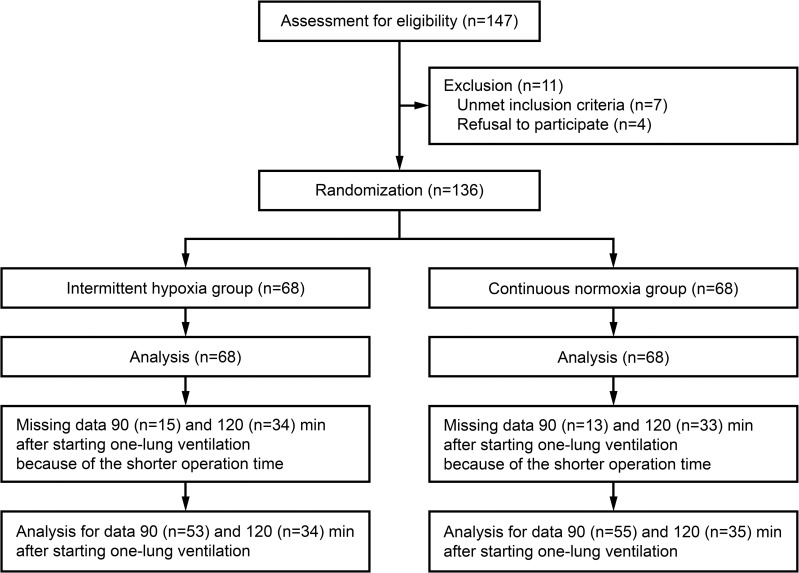
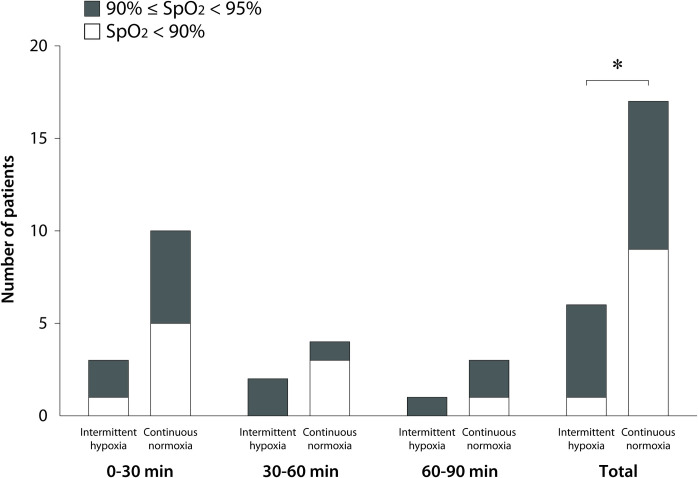
Methods: Patients undergoing one-lung ventilation were randomized into two groups (n = 68 each). Before one-lung ventilation, in the intermittent hypoxia group, the nondependent lung was not ventilated for 2 min and then ventilated for 2 min while the dependent lung was continuously ventilated. This was repeated five times. In the continuous normoxia group, both lungs were ventilated for 20 min. We measured SpO2, PaO2, FiO2, PaCO2, SaO2, and central venous oxygen saturation during one-lung ventilation. The primary outcome was the number of patients with hypoxemia defined as a SpO2 <95% during one-lung ventilation, which was analyzed with a chi-squared test.
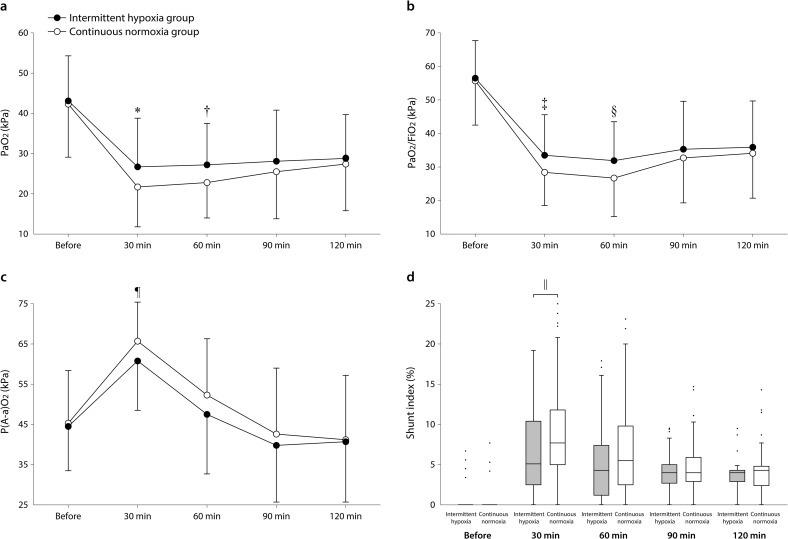
Results: Hypoxemia was less frequent in the intermittent hypoxia group than in the continuous normoxia group during OLV [6/68 (8.8%) vs 17/68 (25.0%), risk ratio (95% CI) 0.35 (0.15-0.84), p = 0.012]. The PaO2 (p = 0.008 for 30 min and 0.007 for 60 min) and PaO2/FiO2 (p = 0.008 for both) were higher 30 and 60 min after starting one-lung ventilation, and the alveolar-arterial pressure gradient (p = 0.010) and shunt index (p = 0.008) were lower 30 min after starting one-lung ventilation in the intermittent hypoxia group than in the continuous normoxia group. Postoperative adverse events did not differ significantly between groups.
Conclusions: Repeated intermittent hypoxic stimuli to the operative lung seemed to potentiate hypoxic pulmonary vasoconstriction, and thus reduced hypoxemia during the subsequent one-lung ventilation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
