

Deep sequencing of DNA from urine of kidney allograft recipients to estimate donor/recipient-specific DNA fractions
- PMID: 33857204
- PMCID: PMC8049329
- DOI: 10.1371/journal.pone.0249930
Deep sequencing of DNA from urine of kidney allograft recipients to estimate donor/recipient-specific DNA fractions
Abstract
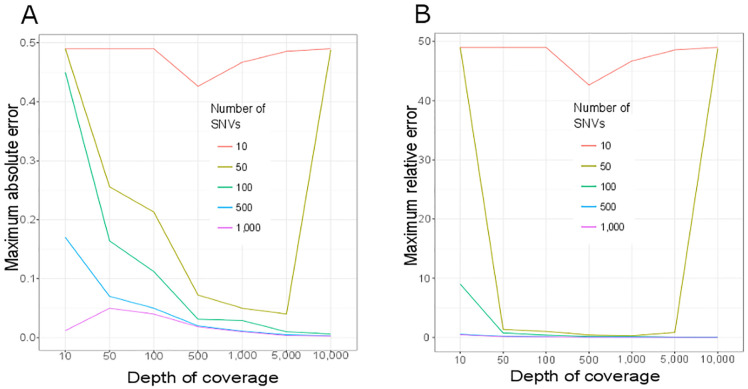
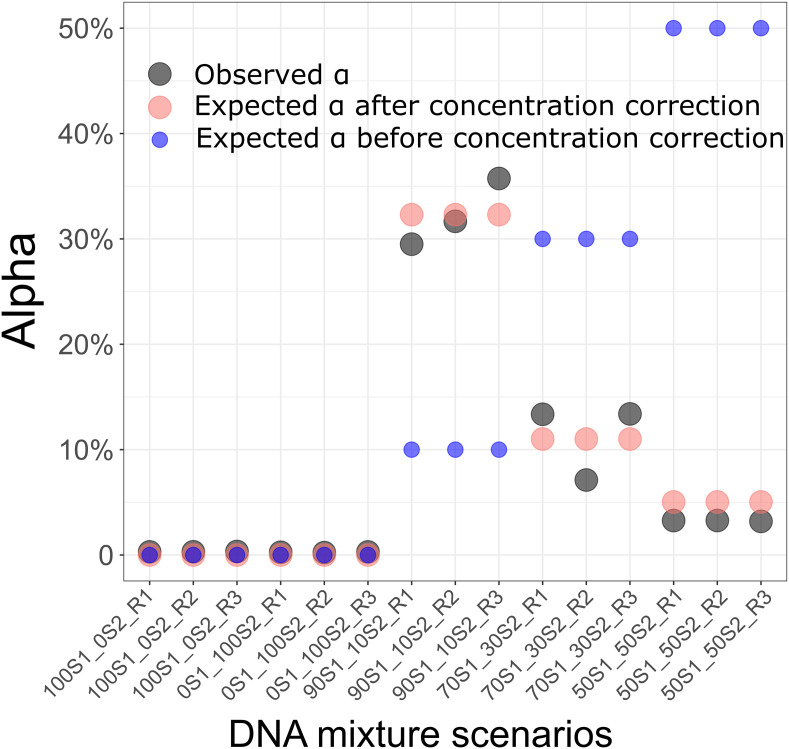
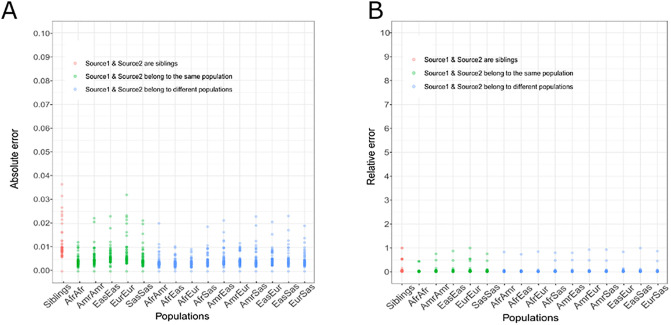
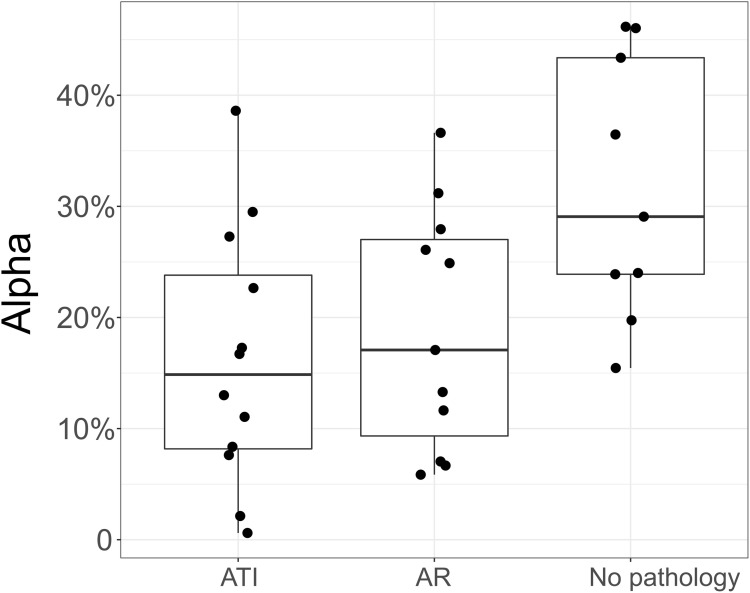
Kidney transplantation is the treatment of choice for patients with end-stage kidney failure, but transplanted allograft could be affected by viral and bacterial infections and by immune rejection. The standard test for the diagnosis of acute pathologies in kidney transplants is kidney biopsy. However, noninvasive tests would be desirable. Various methods using different techniques have been developed by the transplantation community. But these methods require improvements. We present here a cost-effective method for kidney rejection diagnosis that estimates donor/recipient-specific DNA fraction in recipient urine by sequencing urinary cell DNA. We hypothesized that in the no-pathology stage, the largest tissue types present in recipient urine are donor kidney cells, and in case of rejection, a larger number of recipient immune cells would be observed. Extensive in-silico simulation was used to tune the sequencing parameters: number of variants and depth of coverage. Sequencing of DNA mixture from 2 healthy individuals showed the method is highly predictive (maximum error < 0.04). We then demonstrated the insignificant impact of familial relationship and ethnicity using an in-house and public database. Lastly, we performed deep DNA sequencing of urinary cell pellets from 32 biopsy-matched samples representing two pathology groups: acute rejection (AR, 11 samples) and acute tubular injury (ATI, 12 samples) and 9 samples with no pathology. We found a significant association between the donor/recipient-specific DNA fraction in the two pathology groups compared to no pathology (P = 0.0064 for AR and P = 0.026 for ATI). We conclude that deep DNA sequencing of urinary cells from kidney allograft recipients offers a noninvasive means of diagnosing acute pathologies in the human kidney allograft.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
