

Synthetic lethality-mediated precision oncology via the tumor transcriptome
- PMID: 33857424
- PMCID: PMC9310669
- DOI: 10.1016/j.cell.2021.03.030
Synthetic lethality-mediated precision oncology via the tumor transcriptome
Abstract
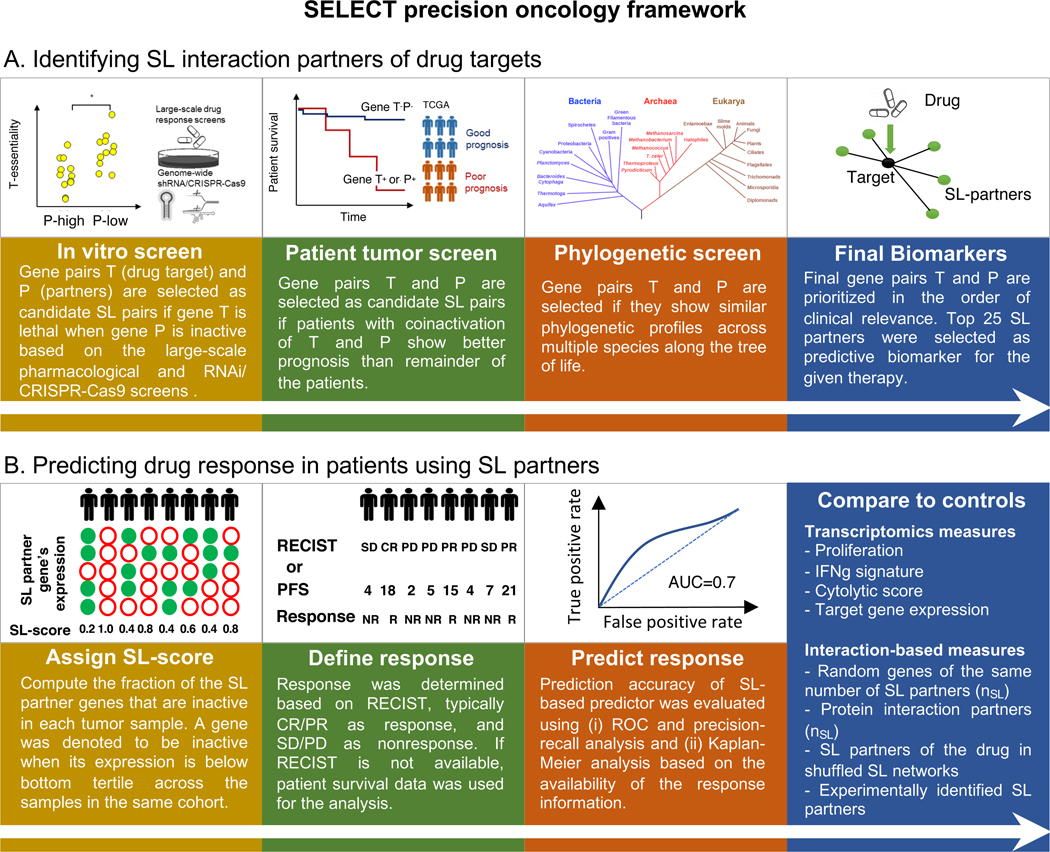
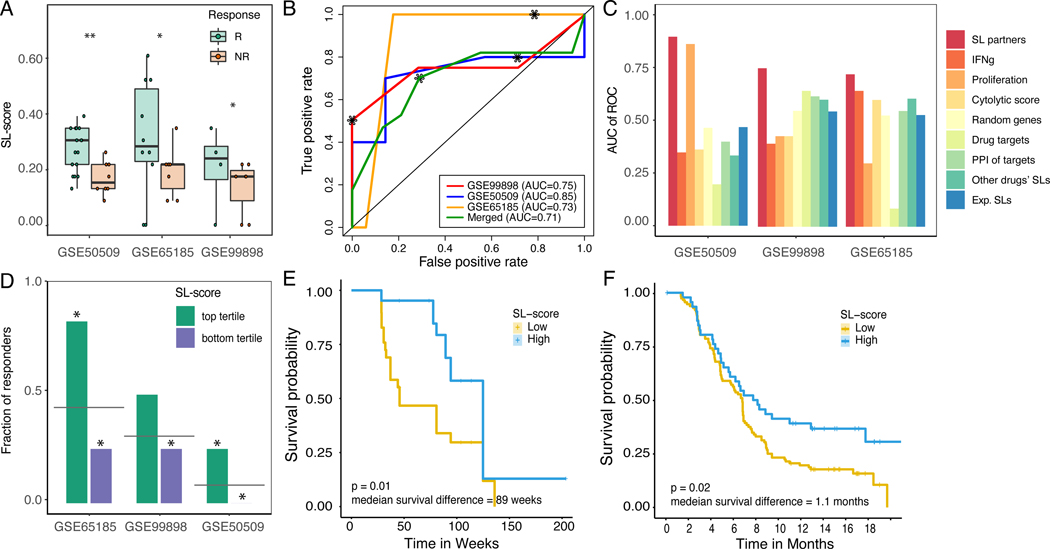
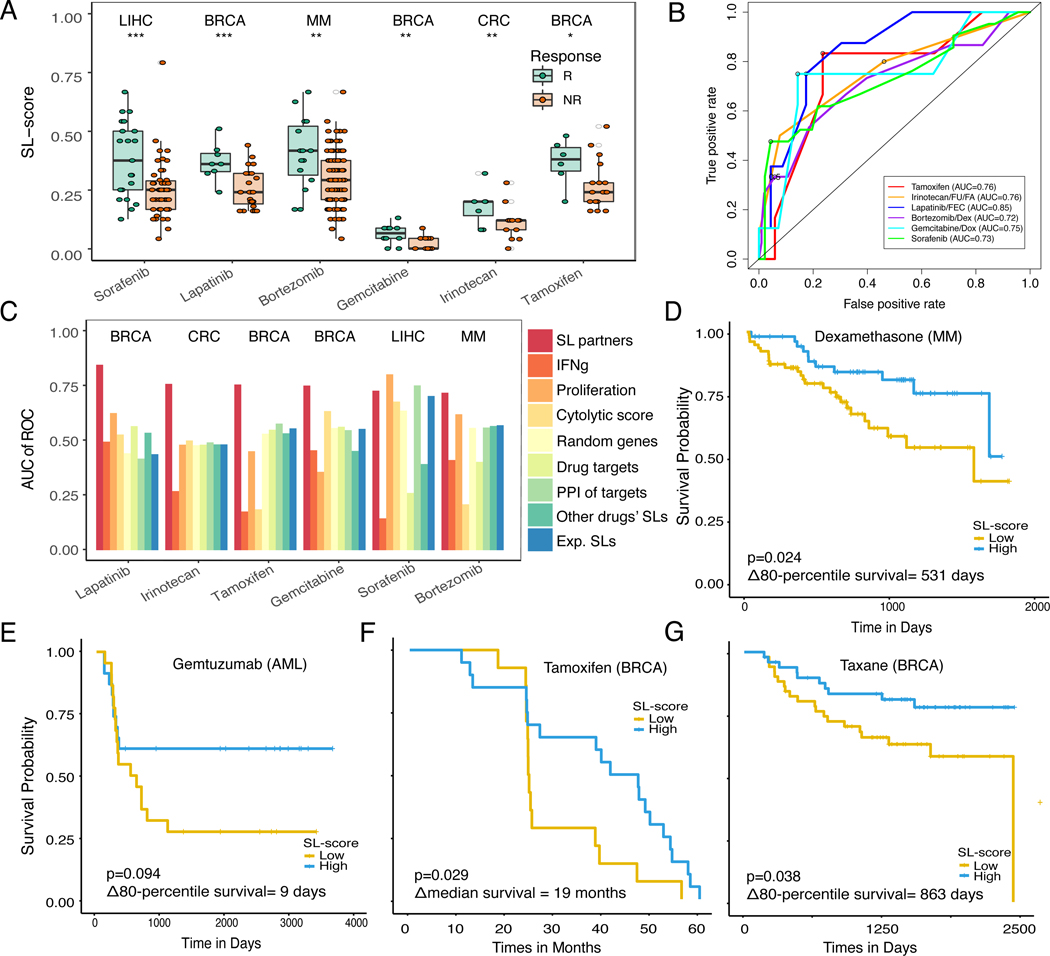
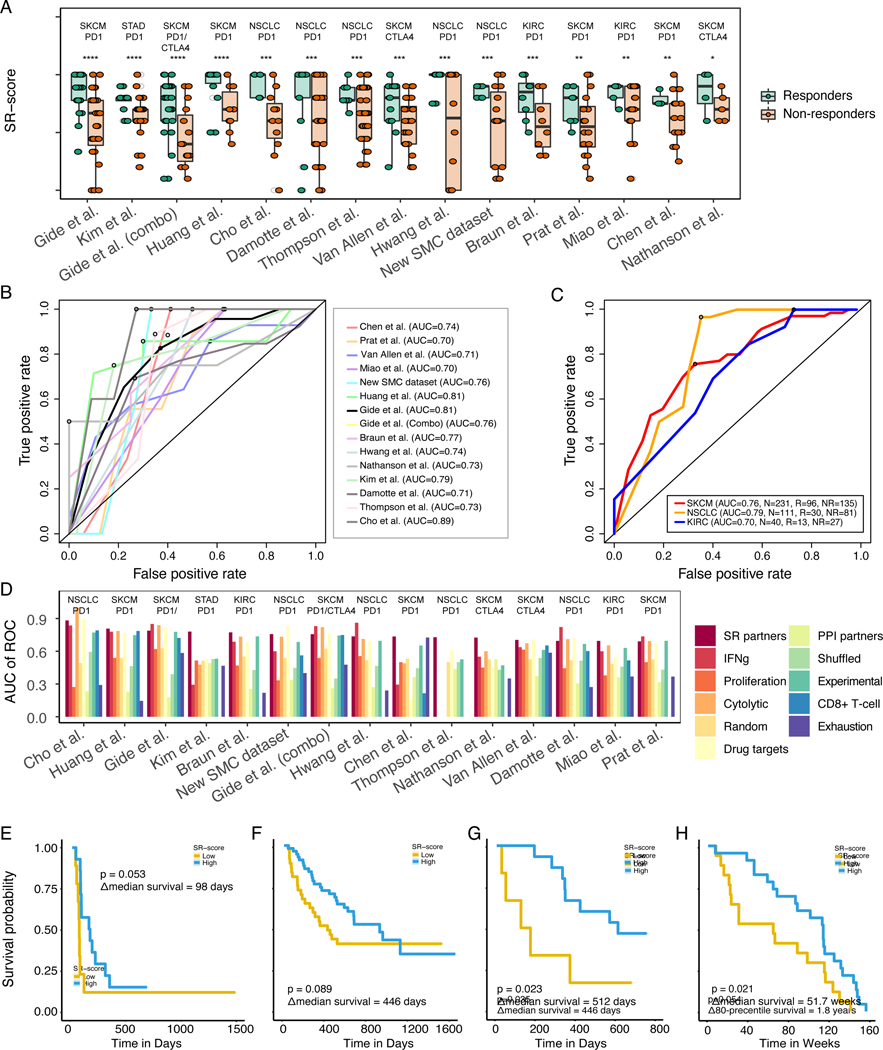
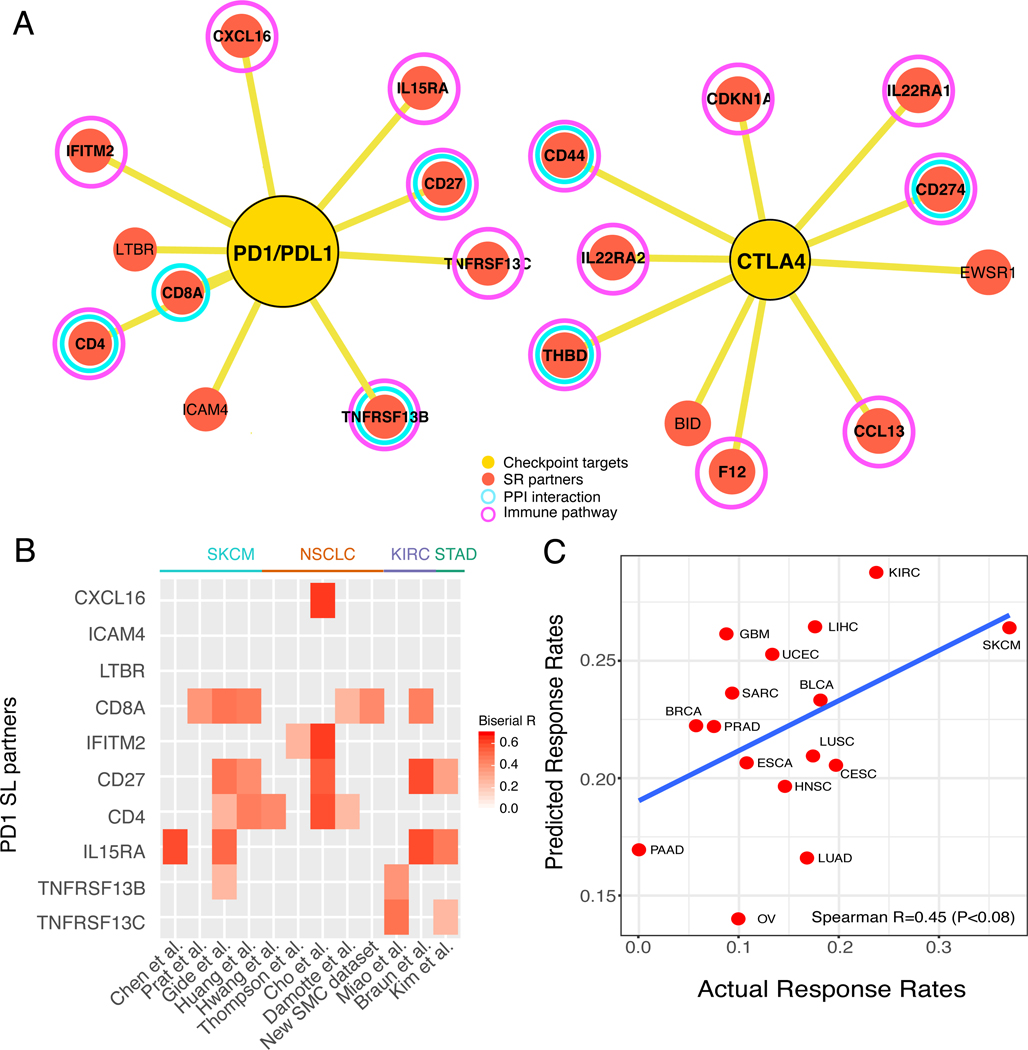
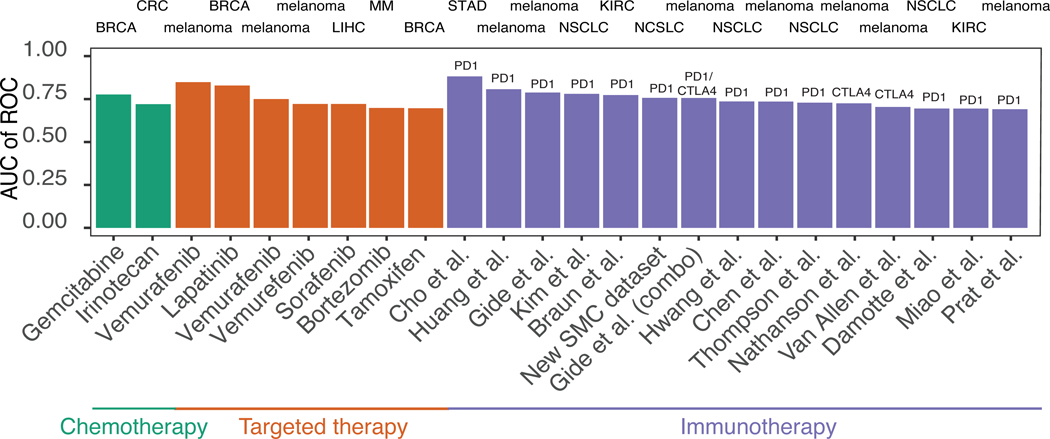
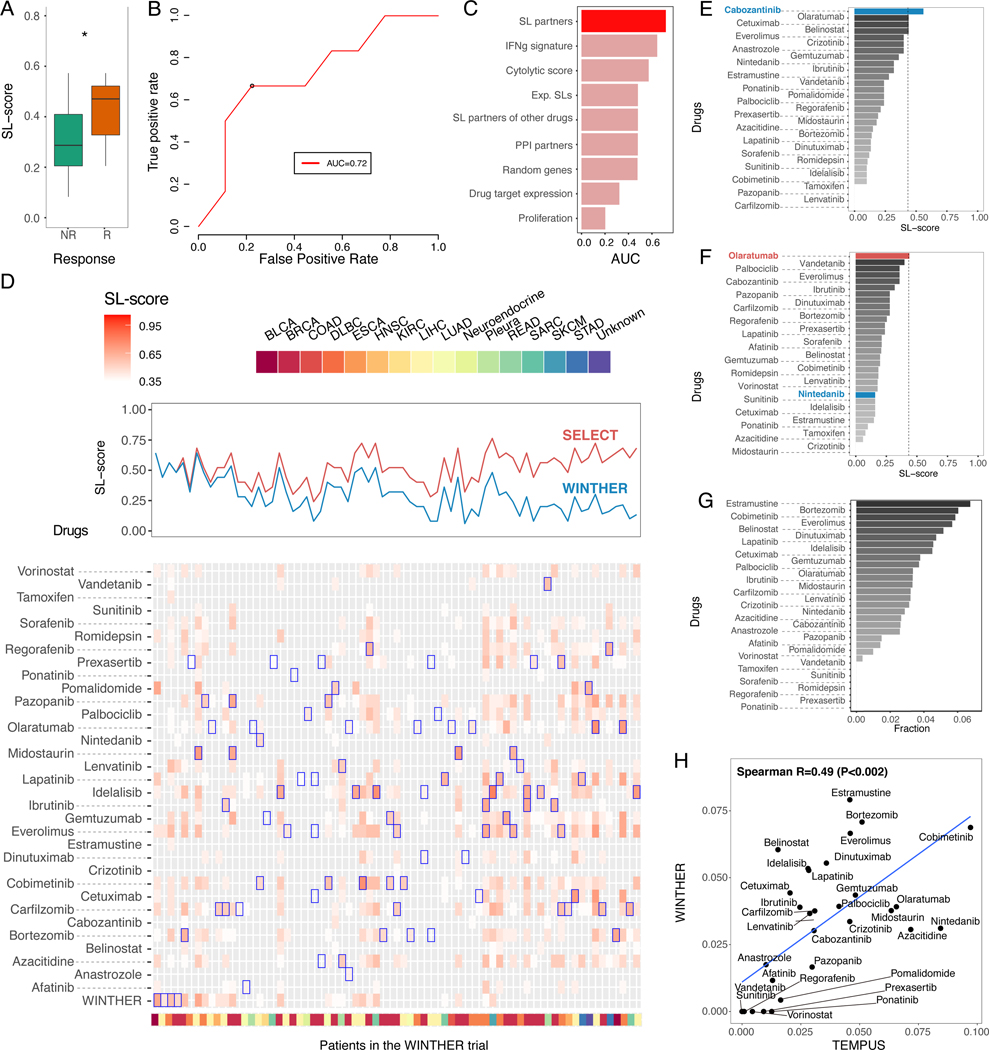
Precision oncology has made significant advances, mainly by targeting actionable mutations in cancer driver genes. Aiming to expand treatment opportunities, recent studies have begun to explore the utility of tumor transcriptome to guide patient treatment. Here, we introduce SELECT (synthetic lethality and rescue-mediated precision oncology via the transcriptome), a precision oncology framework harnessing genetic interactions to predict patient response to cancer therapy from the tumor transcriptome. SELECT is tested on a broad collection of 35 published targeted and immunotherapy clinical trials from 10 different cancer types. It is predictive of patients' response in 80% of these clinical trials and in the recent multi-arm WINTHER trial. The predictive signatures and the code are made publicly available for academic use, laying a basis for future prospective clinical studies.
Keywords: cancer immunotherapy; patient stratification; precision oncology; synthetic lethality; synthetic rescues; transcriptomics.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests E.R. is a co-founder of Medaware, Metabomed, and Pangea Therapeutics (divested from the latter). E.R. serves as a non-paid scientific consultant to Pangea Therapeutics, a company developing a precision oncology SL-based multi-omics approach. J.S.L. is a scientific consultant; T.B. is chief executive officer and chief technical officer; G.D. is head of research and development; R.B. is a member of the Scientific Advisory Board; and Z.R. is a co-founder and a scientific advisor at Pangea Therapeutics. R.K. receives research funding from Genentech, Merck Serono, Pfizer, Boehringer Ingelheim, TopAlliance, Takeda, Incyte, Debiopharm, Medimmune, Sequenom, Foundation Medicine, Konica Minolta, Grifols, Omniseq, and Guardant; received consultant, speaker, and/or advisory board fees for X-Biotech, Neomed, Pfizer, Actuate Therapeutics, Roche, Turning Point Therapeutics, TD2/Volastra, and Bicara Therapeutics; has an equity interest in IDbyDNA and CureMatch; serves on the board of CureMatch and CureMetrix; and is a co-founder of CureMatch. A patent application associated with this manuscript is in process.
Figures
References
-
- Beaubier N, Bontrager M, Huether R, Igartua C, Lau D, Tell R, Bobe AM, Bush S, Chang AL, Hoskinson DC, et al. (2019). Integrated genomic profiling expands clinical options for patients with cancer. Nat Biotechnol. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
