

Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses
- PMID: 33857435
- PMCID: PMC8041436
- DOI: 10.1016/S2213-2600(21)00125-9
Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses
Abstract
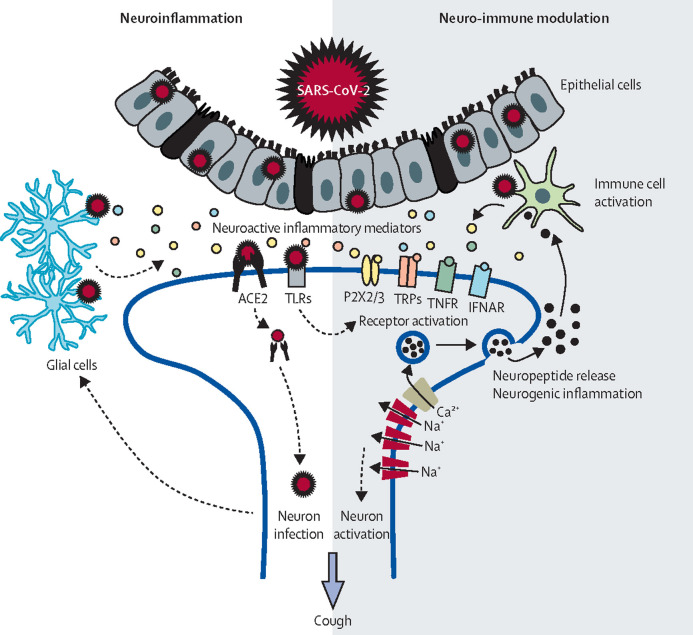
Cough is one of the most common presenting symptoms of COVID-19, along with fever and loss of taste and smell. Cough can persist for weeks or months after SARS-CoV-2 infection, often accompanied by chronic fatigue, cognitive impairment, dyspnoea, or pain-a collection of long-term effects referred to as the post-COVID syndrome or long COVID. We hypothesise that the pathways of neurotropism, neuroinflammation, and neuroimmunomodulation through the vagal sensory nerves, which are implicated in SARS-CoV-2 infection, lead to a cough hypersensitivity state. The post-COVID syndrome might also result from neuroinflammatory events in the brain. We highlight gaps in understanding of the mechanisms of acute and chronic COVID-19-associated cough and post-COVID syndrome, consider potential ways to reduce the effect of COVID-19 by controlling cough, and suggest future directions for research and clinical practice. Although neuromodulators such as gabapentin or opioids might be considered for acute and chronic COVID-19 cough, we discuss the possible mechanisms of COVID-19-associated cough and the promise of new anti-inflammatories or neuromodulators that might successfully target both the cough of COVID-19 and the post-COVID syndrome.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests KFC has received honoraria for participating in advisory board meetings for GlaxoSmithKline, AstraZeneca, Novartis, Merck, Boehringer Ingelheim, Nocion, Shionogi, Roche, and TEVA Pharmaceutical regarding treatments for asthma and chronic obstructive pulmonary disease; he has recieved honoraria for participating on the scientific advisory board of the Clean Breathing Institute, supported by GlaxoSmithKline Health Care Consumer Products; and he has been remunerated for speaking engagements by AstraZeneca, Novartis, and Merck. SBM reports grants from Merck and personal fees from Merck and NeRRe Therapeutics. SSB reports personal fees from Nocion, Merck, Nerre, Bayer, Bellus, and Shionogi; and grants from Merck, all outside the submitted work. LM reports personal fees from GlaxoSmithKline, Merck, Shionogi, Bayer, Bellus Health, Nocion, Chiesi, and Applied Clinical Intelligence; and grants from Merck and Chesi, all outside the submitted work. JHH has received grant funding and advisory fees from MSD pharmaceuticals and is a member of the advisory board for Bellus health. The other authors declare no competing interests.
Figures
References
-
- Hulme K, Dogan S, Parker SM, Deary V. ‘Chronic cough, cause unknown’: A qualitative study of patient perspectives of chronic refractory cough. J Health Psychol. 2019;24:707–716. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
