

Hospital-Acquired Infections in Critically Ill Patients With COVID-19
- PMID: 33857475
- PMCID: PMC8056844
- DOI: 10.1016/j.chest.2021.04.002
Hospital-Acquired Infections in Critically Ill Patients With COVID-19
Abstract
Background: Few small studies have described hospital-acquired infections (HAIs) occurring in patients with COVID-19.
Research question: What characteristics in critically ill patients with COVID-19 are associated with HAIs and how are HAIs associated with outcomes in these patients?
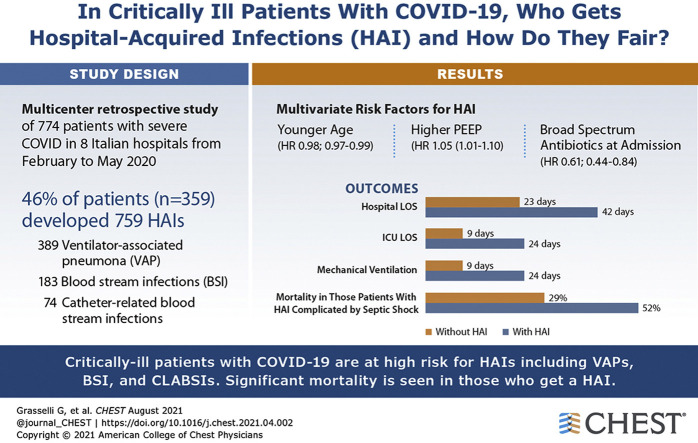
Study design and methods: Multicenter retrospective analysis of prospectively collected data including adult patients with severe COVID-19 admitted to eight Italian hub hospitals from February 20, 2020, through May 20, 2020. Descriptive statistics and univariate and multivariate Weibull regression models were used to assess incidence, microbial cause, resistance patterns, risk factors (ie, demographics, comorbidities, exposure to medication), and impact on outcomes (ie, ICU discharge, length of ICU and hospital stays, and duration of mechanical ventilation) of microbiologically confirmed HAIs.
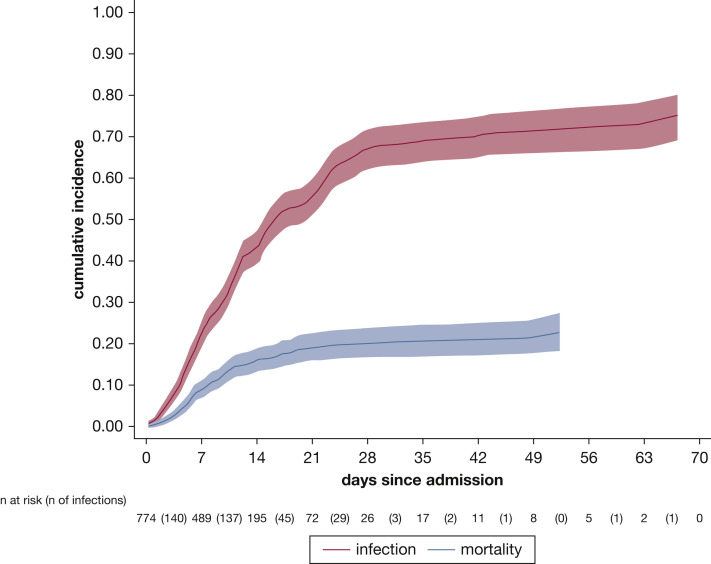
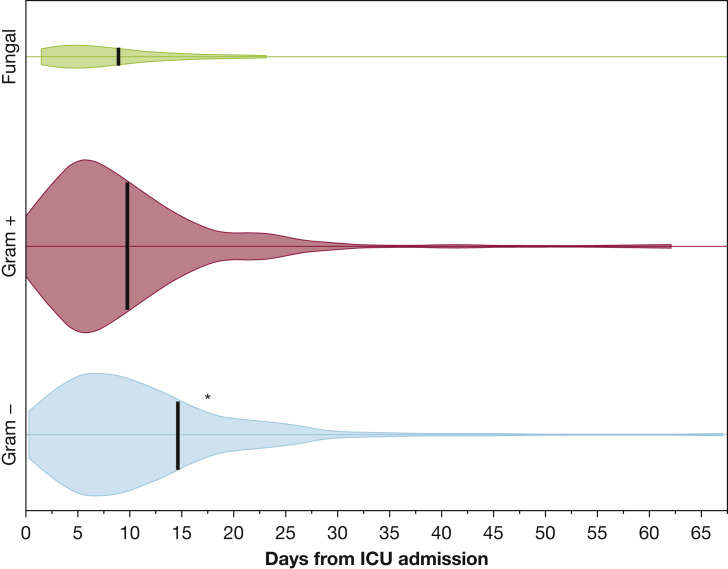
Results: Of the 774 included patients, 359 patients (46%) demonstrated 759 HAIs (44.7 infections/1,000 ICU patient-days; 35% multidrug-resistant [MDR] bacteria). Ventilator-associated pneumonia (VAP; n = 389 [50%]), bloodstream infections (BSIs; n = 183 [34%]), and catheter-related BSIs (n = 74 [10%]) were the most frequent HAIs, with 26.0 (95% CI, 23.6-28.8) VAPs per 1,000 intubation-days, 11.7 (95% CI, 10.1-13.5) BSIs per 1,000 ICU patient-days, and 4.7 (95% CI, 3.8-5.9) catheter-related BSIs per 1,000 ICU patient-days. Gram-negative bacteria (especially Enterobacterales) and Staphylococcus aureus caused 64% and 28% of cases of VAP, respectively. Variables independently associated with infection were age, positive end expiratory pressure, and treatment with broad-spectrum antibiotics at admission. Two hundred thirty-four patients (30%) died in the ICU (15.3 deaths/1,000 ICU patient-days). Patients with HAIs complicated by septic shock showed an almost doubled mortality rate (52% vs 29%), whereas noncomplicated infections did not affect mortality. HAIs prolonged mechanical ventilation (median, 24 days [interquartile range (IQR), 14-39 days] vs 9 days [IQR, 5-13 days]; P < .001), ICU stay (24 days [IQR, 16-41 days] vs 9 days [IQR, 6-14 days]; P = .003), and hospital stay (42 days [IQR, 25-59 days] vs 23 days [IQR, 13-34 days]; P < .001).
Interpretation: Critically ill patients with COVID-19 are at high risk for HAIs, especially VAPs and BSIs resulting from MDR organisms. HAIs prolong mechanical ventilation and hospitalization, and HAIs complicated by septic shock almost double mortality.
Trial registry: ClinicalTrials.gov; No.: NCT04388670; URL: www.clinicaltrials.gov.
Keywords: COVID-19; SARS-CoV-2; critical care; hospital-acquired infections.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Elephant in the Room: Secondary Infections and Antimicrobial Use in Patients With COVID-19.Chest. 2021 Aug;160(2):387-388. doi: 10.1016/j.chest.2021.04.053. Chest. 2021. PMID: 34366018 Free PMC article. No abstract available.
-
High Incidence of Nosocomial Infections in COVID-19 Patients: Is SARS-CoV-2 the Culprit?Chest. 2021 Sep;160(3):e315. doi: 10.1016/j.chest.2021.04.074. Chest. 2021. PMID: 34488975 Free PMC article. No abstract available.
-
Response.Chest. 2021 Sep;160(3):e316. doi: 10.1016/j.chest.2021.05.040. Chest. 2021. PMID: 34488976 Free PMC article. No abstract available.
References
-
- Grasselli G., Pesenti A., Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy. JAMA. 2020;323(16):1545–1546. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
