

Biomarkers of Kidney Tubule Health, CKD Progression, and Acute Kidney Injury in SPRINT (Systolic Blood Pressure Intervention Trial) Participants
- PMID: 33857535
- PMCID: PMC8384678
- DOI: 10.1053/j.ajkd.2021.01.021
Biomarkers of Kidney Tubule Health, CKD Progression, and Acute Kidney Injury in SPRINT (Systolic Blood Pressure Intervention Trial) Participants
Abstract
Rationale & objective: The Systolic Blood Pressure Intervention Trial (SPRINT) compared the effect of intensive versus standard systolic blood pressure targets on cardiovascular morbidity and mortality. In this ancillary study, we evaluated the use of exploratory factor analysis (EFA) to combine biomarkers of kidney tubule health in urine and plasma and then study their role in longitudinal estimated glomerular filtration rate (eGFR) change and risk of acute kidney injury (AKI).
Study design: Observational cohort nested in a clinical trial.
Setting & participants: 2,351 SPRINT participants with eGFR < 60 mL/min/1.73 m2 at baseline.
Exposure: Levels of neutrophil gelatinase-associated lipocalin (NGAL), interleukin 18 (IL-18), chitinase-3-like protein (YKL-40), kidney injury molecule 1 (KIM-1), monocyte chemoattractant protein 1 (MCP-1), α1-microglobulin (A1M) and β2-microglobulin (B2M), uromodulin (UMOD), fibroblast growth factor 23 (FGF-23), and intact parathyroid hormone (PTH).
Outcome: Longitudinal changes in eGFR and risk of AKI.
Analytical approach: We performed EFA to capture different tubule pathophysiologic processes. We used linear mixed effects models to evaluate the association of each factor with longitudinal changes in eGFR. We evaluated the association of the tubular factors scores with AKI using Cox proportional hazards regression.
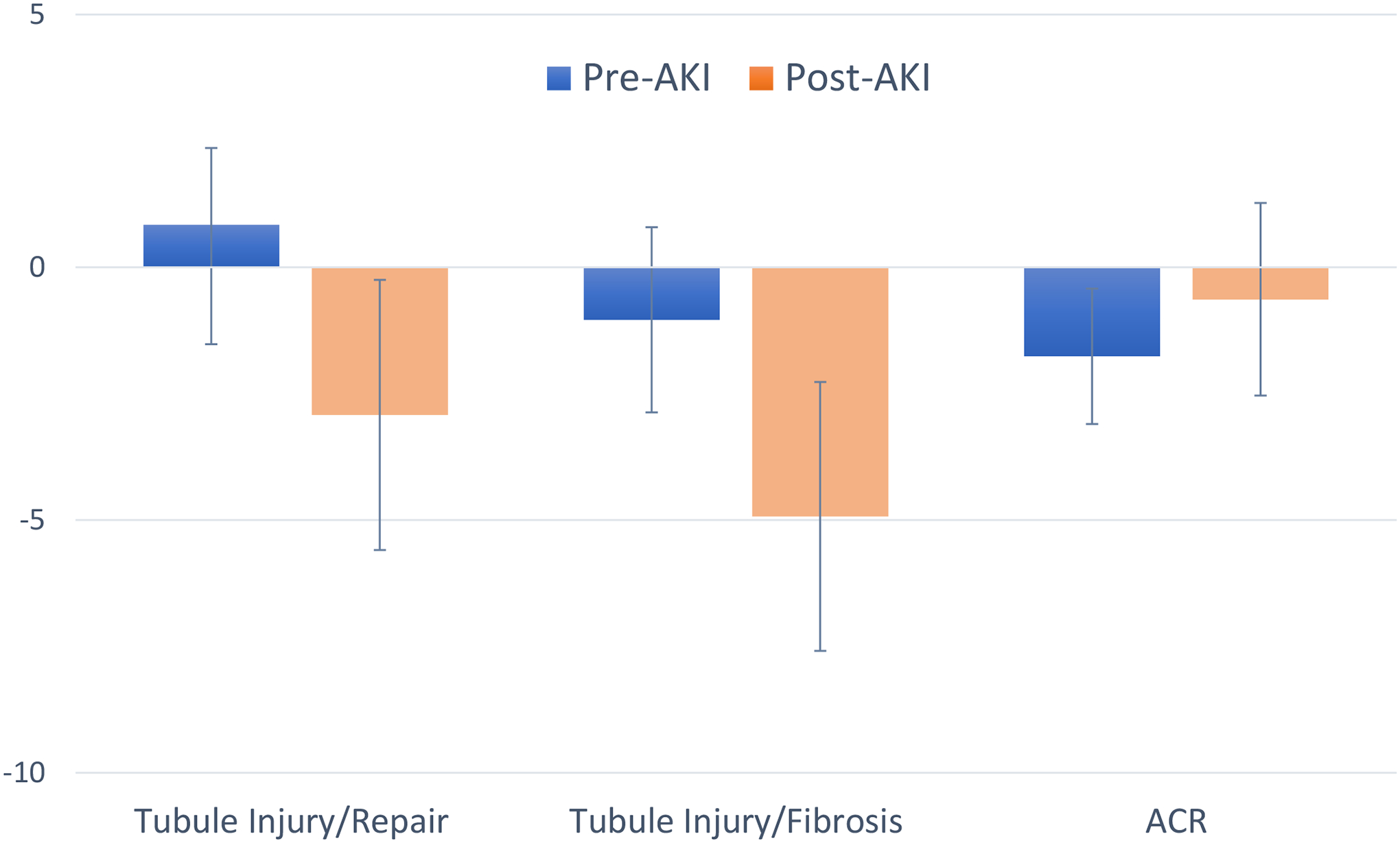
Results: From 10 biomarkers, EFA generated 4 factors reflecting tubule injury/repair (NGAL, IL-18, and YKL-40), tubule injury/fibrosis (KIM-1 and MCP-1), tubule reabsorption (A1M and B2M), and tubule reserve/mineral metabolism (UMOD, FGF-23, and PTH). Each 1-SD higher tubule reserve/mineral metabolism factor score was associated with a 0.58% (95% CI, 0.39%-0.67%) faster eGFR decline independent of baseline eGFR and albuminuria. Both the tubule injury/repair and tubule injury/fibrosis factors were independently associated with future risk of AKI (per 1 SD higher, HRs of 1.18 [95% CI, 1.10-1.37] and 1.23 [95% CI, 1.02-1.48], respectively).
Limitations: The factors require validation in other settings.
Conclusions: EFA allows parsimonious subgrouping of biomarkers into factors that are differentially associated with progressive eGFR decline and AKI. These subgroups may provide insights into the pathological processes driving adverse kidney outcomes.
Keywords: Acute kidney injury (AKI); CKD progression; chronic kidney disease (CKD); eGFR trajectory; estimated glomerular filtration rate (eGFR); kidney tubule; plasma biomarker; renal function; tubular dysfunction; tubular marker; urine biomarker.
Published by Elsevier Inc.
Conflict of interest statement
Financial Disclosure: The authors declare that they have no relevant financial interests.
Figures
Comment in
-
Tubular Kidney Biomarker Insights Through Factor Analysis.Am J Kidney Dis. 2021 Sep;78(3):335-337. doi: 10.1053/j.ajkd.2021.03.016. Epub 2021 May 20. Am J Kidney Dis. 2021. PMID: 34023146 Free PMC article. No abstract available.
References
-
- Golestaneh L, Alvarez PJ, Reaven NL, et al. All-cause costs increase exponentially with increased chronic kidney disease stage. Am J Manag Care. June2017;23(10 Suppl):S163–s172. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
