

Endothelial-Mesenchymal Transition in COVID-19 lung lesions
- PMID: 33857718
- PMCID: PMC7997691
- DOI: 10.1016/j.prp.2021.153419
Endothelial-Mesenchymal Transition in COVID-19 lung lesions
Abstract
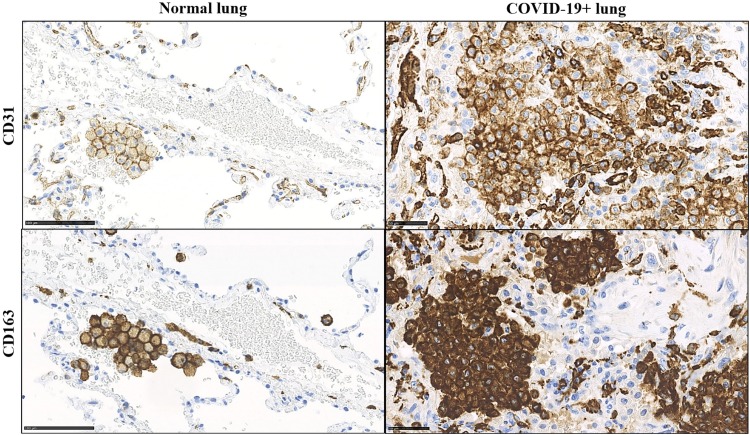
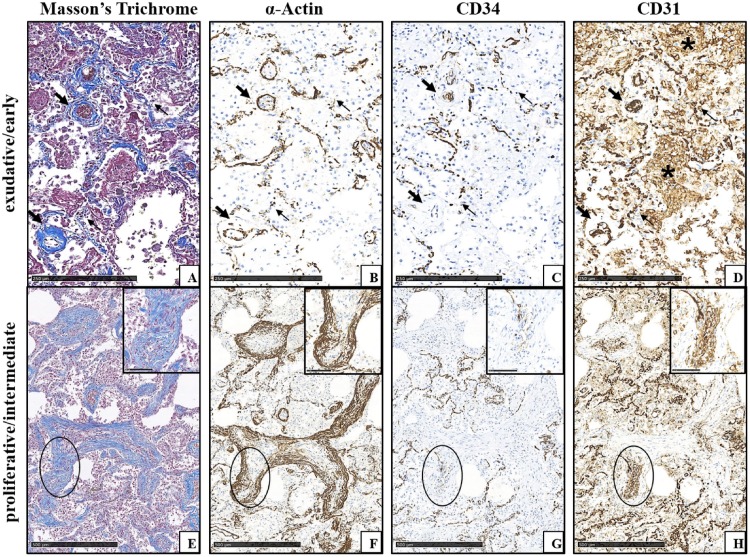
Sars-Cov-2 infection is still a healthcare emergency and acute respiratory distress failure with Diffuse Alveolar Damage (DAD) features is the main causes of patients' death. Pathogenic mechanisms of the disease are not clear yet, but new insights are necessary to improve therapeutic management, to prevent fatal irreversible multi-organ damage and to adequately follow up those patients who survive. Here we investigated, by histochemistry and immunohistochemistry, a wide number of mapped lung specimens taken from whole body autopsies of 7 patients dead of COVID-19 disease. Our data confirm morphological data of other authors, and enlarge recent reports of the literature suggesting that Endothelial-Mesenchymal Transition might be central to COVID-19 lung fibrosing lesions. Furthermore, based upon recent acquisition of new roles in immunity and vascular pathology of the CD31 molecule, we hypothesize that this molecule might be important in the development and treatment of COVID-19 pulmonary lesions. These preliminary findings need further investigations to shed light on the complexity of Sars-Cov-2 disease.
Keywords: CD31; COVID-19; Diffuse alveolar damage; Endothelial-Mesenchymal Transition; Fibrosis.
Copyright © 2021 Elsevier GmbH. All rights reserved.
Conflict of interest statement
The authors report no declarations of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
