

Clinical metagenomics assessments improve diagnosis and outcomes in community-acquired pneumonia
- PMID: 33858378
- PMCID: PMC8047593
- DOI: 10.1186/s12879-021-06039-1
Clinical metagenomics assessments improve diagnosis and outcomes in community-acquired pneumonia
Abstract
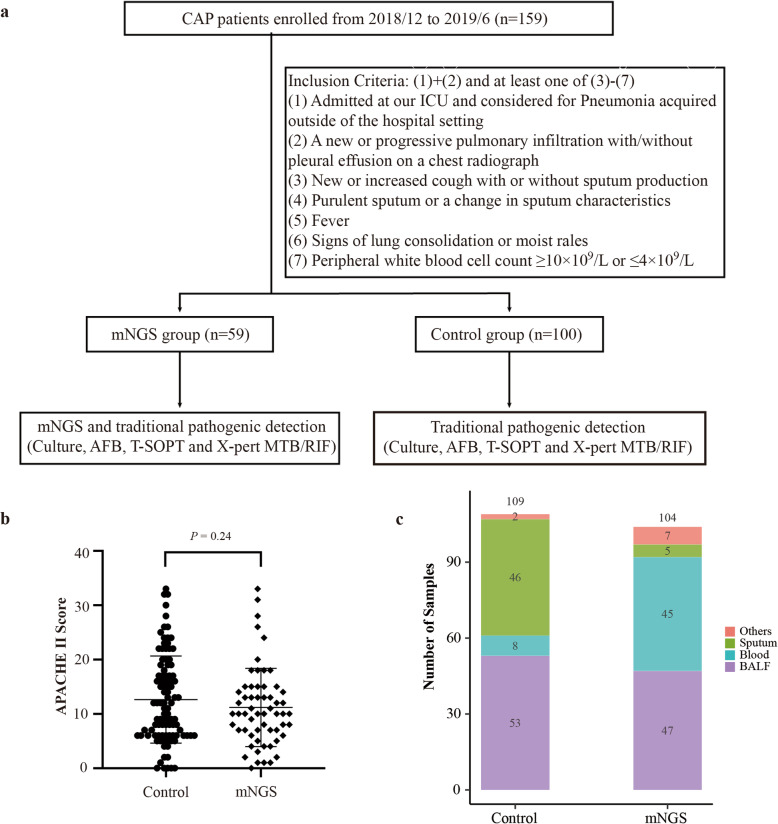
Background: Identifying the causes of community-acquired pneumonia (CAP) is challenging due to the disease's complex etiology and the limitations of traditional microbiological diagnostic methods. Recent advances in next generation sequencing (NGS)-based metagenomics allow pan-pathogen detection in a single assay, and may have significant advantages over culture-based techniques.
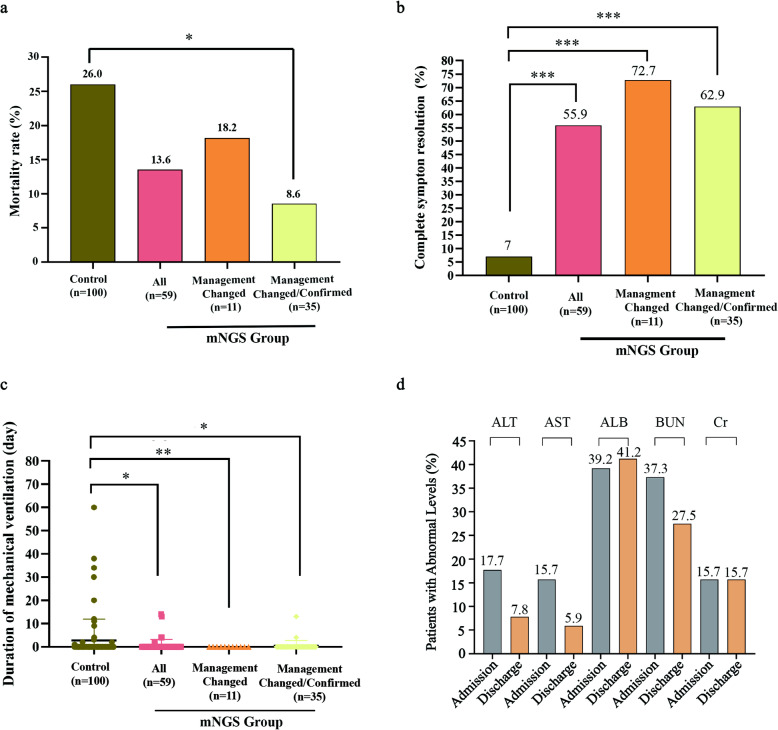
Results: We conducted a cohort study of 159 CAP patients to assess the diagnostic performance of a clinical metagenomics assay and its impact on clinical management and patient outcomes. When compared to other techniques, clinical metagenomics detected more pathogens in more CAP cases, and identified a substantial number of polymicrobial infections. Moreover, metagenomics results led to changes in or confirmation of clinical management in 35 of 59 cases; these 35 cases also had significantly improved patient outcomes.
Conclusions: Clinical metagenomics could be a valuable tool for the diagnosis and treatment of CAP.
Trial registration: Trial registration number with the Chinese Clinical Trial Registry: ChiCTR2100043628 .
Keywords: Clinical metagenomics; Clinical study; Community-acquired pneumonia; Next-generation sequencing; Polymicrobial infections.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures

Similar articles
-
The etiological diagnostic value of metagenomic next-generation sequencing in suspected community-acquired pneumonia.BMC Infect Dis. 2024 Jun 24;24(1):626. doi: 10.1186/s12879-024-09507-6. BMC Infect Dis. 2024. PMID: 38914949 Free PMC article.
-
Metagenomics in the Diagnosis of Pneumonia: Protocol for a Systematic Review.JMIR Res Protoc. 2024 Sep 18;13:e57334. doi: 10.2196/57334. JMIR Res Protoc. 2024. PMID: 39293053 Free PMC article.
-
Microbiological diagnostic performance of metagenomic next-generation sequencing compared with conventional culture for patients with community-acquired pneumonia.Front Cell Infect Microbiol. 2023 Mar 16;13:1136588. doi: 10.3389/fcimb.2023.1136588. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37009509 Free PMC article.
-
Etiology of community-acquired pneumonia.Clin Chest Med. 2005 Mar;26(1):47-55. doi: 10.1016/j.ccm.2004.10.016. Clin Chest Med. 2005. PMID: 15802165 Free PMC article. Review.
-
Usefulness of sputum gram stain for etiologic diagnosis in community-acquired pneumonia: a systematic review and meta-analysis.BMC Infect Dis. 2019 May 10;19(1):403. doi: 10.1186/s12879-019-4048-6. BMC Infect Dis. 2019. PMID: 31077143 Free PMC article.
Cited by
-
COVID-19 diagnostic approaches with an extensive focus on computed tomography in accurate diagnosis, prognosis, staging, and follow-up.Pol J Radiol. 2023 Jan 27;88:e53-e64. doi: 10.5114/pjr.2023.124597. eCollection 2023. Pol J Radiol. 2023. PMID: 36819223 Free PMC article. Review.
-
Evaluation of Metagenomic and Targeted Next-Generation Sequencing Workflows for Detection of Respiratory Pathogens from Bronchoalveolar Lavage Fluid Specimens.J Clin Microbiol. 2022 Jul 20;60(7):e0052622. doi: 10.1128/jcm.00526-22. Epub 2022 Jun 13. J Clin Microbiol. 2022. PMID: 35695488 Free PMC article.
-
Clinical characteristics and outcomes of immunocompromised patients with severe community-acquired pneumonia: A single-center retrospective cohort study.Front Public Health. 2023 Feb 15;11:1070581. doi: 10.3389/fpubh.2023.1070581. eCollection 2023. Front Public Health. 2023. PMID: 36875372 Free PMC article.
-
Pathogen profiling of Australian rabbits by metatranscriptomic sequencing.Transbound Emerg Dis. 2022 Sep;69(5):e2629-e2640. doi: 10.1111/tbed.14609. Epub 2022 Jun 22. Transbound Emerg Dis. 2022. PMID: 35687756 Free PMC article.
-
Yield of clinical metagenomics: insights from real-world practice for tissue infections.EBioMedicine. 2025 Jan;111:105536. doi: 10.1016/j.ebiom.2024.105536. Epub 2024 Dec 26. EBioMedicine. 2025. PMID: 39729886 Free PMC article.
References
-
- Polverino, ETorres Marti, A. Community-acquired pneumonia. Minerva Anestesiol. 2011;77:196–211. - PubMed
-
- Jain S, Self WH, Wunderink RG, Fakhran S, Balk R, Bramley AM, Reed C, Grijalva CG, Anderson EJ, Courtney DM, Chappell JD, Qi C, Hart EM, Carroll F, Trabue C, Donnelly HK, Williams DJ, Zhu Y, Arnold SR, Ampofo K, Waterer GW, Levine M, Lindstrom S, Winchell JM, Katz JM, Erdman D, Schneider E, Hicks LA, McCullers J, Pavia AT, Edwards KM, Finelli L, CDC EPIC Study Team Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N Engl J Med. 2015;373(5):415–427. doi: 10.1056/NEJMoa1500245. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
