

Establishment and validation of a prognostic signature for lung adenocarcinoma based on metabolism-related genes
- PMID: 33858449
- PMCID: PMC8050921
- DOI: 10.1186/s12935-021-01915-x
Establishment and validation of a prognostic signature for lung adenocarcinoma based on metabolism-related genes
Erratum in
-
Correction: Establishment and validation of a prognostic signature for lung adenocarcinoma based on metabolism-related genes.Cancer Cell Int. 2025 Dec 23;25(1):438. doi: 10.1186/s12935-025-04116-y. Cancer Cell Int. 2025. PMID: 41430674 Free PMC article. No abstract available.
Abstract
Background: Given that dysregulated metabolism has been recently identified as a hallmark of cancer biology, this study aims to establish and validate a prognostic signature of lung adenocarcinoma (LUAD) based on metabolism-related genes (MRGs).
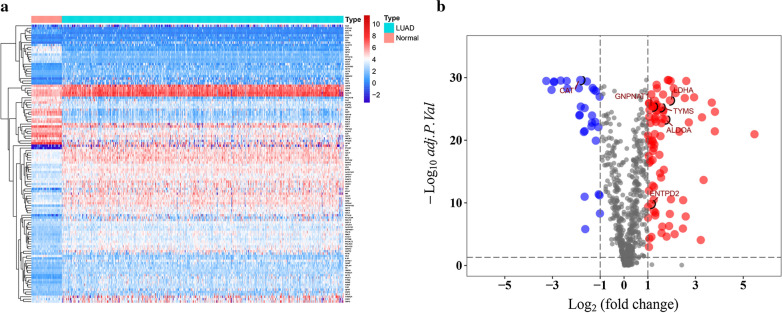
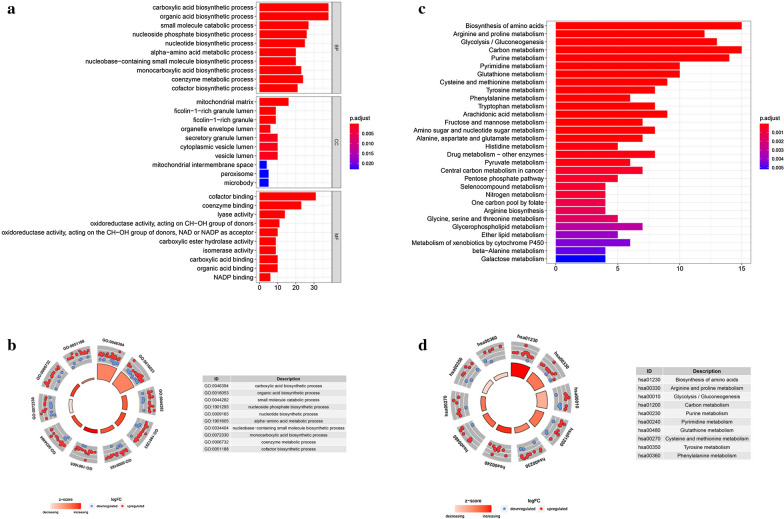
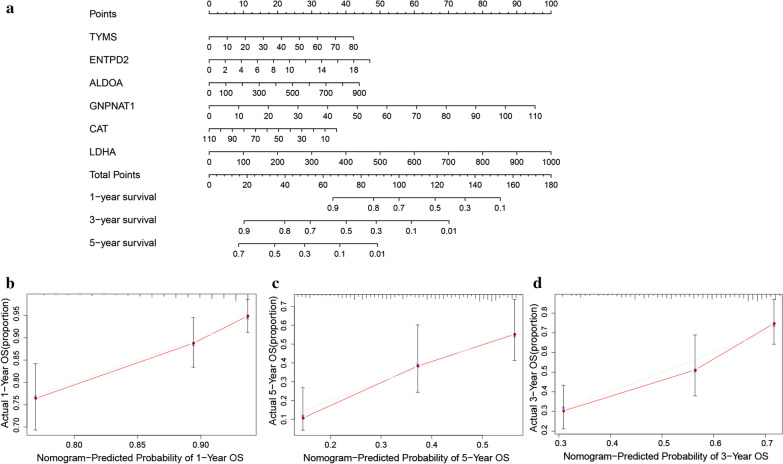
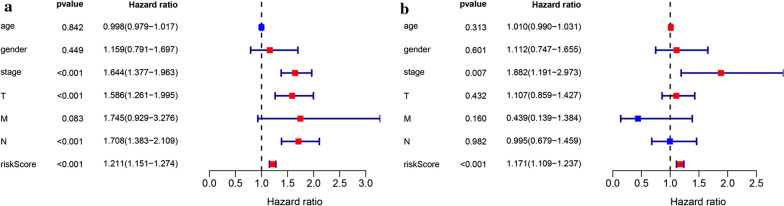
Methods: The gene sequencing data of LUAD samples with clinical information and the metabolism-related gene set were obtained from The Cancer Genome Atlas (TCGA) and Molecular Signatures Database (MSigDB), respectively. The differentially expressed MRGs were identified by Wilcoxon rank sum test. Then, univariate cox regression analysis was performed to identify MRGs that related to overall survival (OS). A prognostic signature was developed by multivariate Cox regression analysis. Furthermore, the signature was validated in the GSE31210 dataset. In addition, a nomogram that combined the prognostic signature was created for predicting the 1-, 3- and 5-year OS of LUAD. The accuracy of the nomogram prediction was evaluated using a calibration plot. Finally, cox regression analysis was applied to identify the prognostic value and clinical relationship of the signature in LUAD.
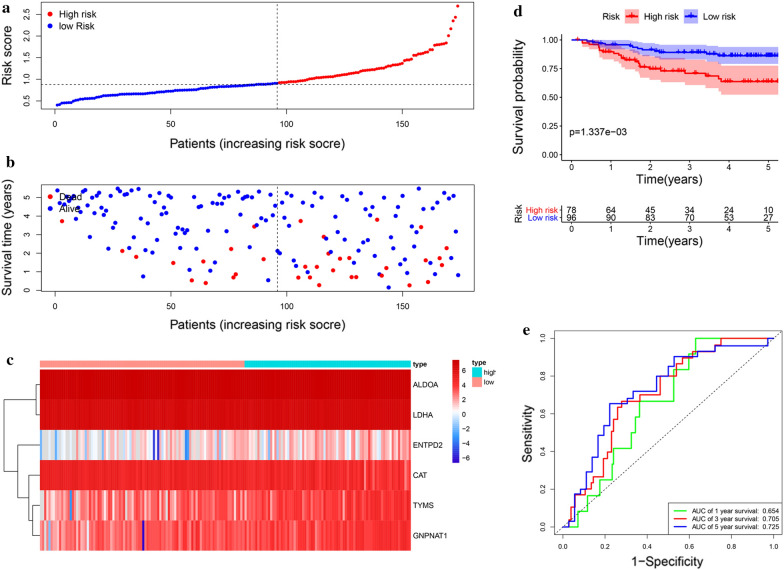
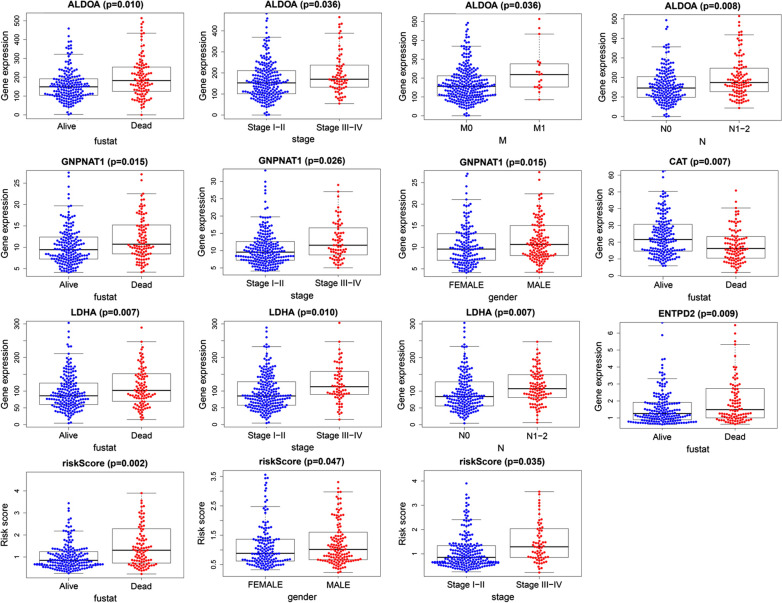
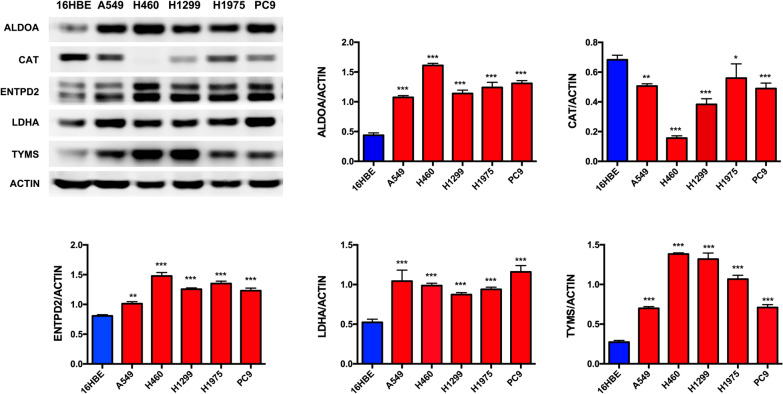
Results: A total of 116 differentially expressed MRGs were detected in the TCGA dataset. We found that 12 MRGs were most significantly associated with OS by using the univariate regression analysis in LUAD. Then, multivariate Cox regression analyses were applied to construct the prognostic signature, which consisted of six MRGs-aldolase A (ALDOA), catalase (CAT), ectonucleoside triphosphate diphosphohydrolase-2 (ENTPD2), glucosamine-phosphate N-acetyltransferase 1 (GNPNAT1), lactate dehydrogenase A (LDHA), and thymidylate synthetase (TYMS). The prognostic value of this signature was further successfully validated in the GSE31210 dataset. Furthermore, the calibration curve of the prognostic nomogram demonstrated good agreement between the predicted and observed survival rates for each of OS. Further analysis indicated that this signature could be an independent prognostic indicator after adjusting to other clinical factors. The high-risk group patients have higher levels of immune checkpoint molecules and are therefore more sensitive to immunotherapy. Finally, we confirmed six MRGs protein and mRNA expression in six lung cancer cell lines and firstly found that ENTPD2 might played an important role on LUAD cells colon formation and migration.
Conclusions: We established a prognostic signature based on MRGs for LUAD and validated the performance of the model, which may provide a promising tool for the diagnosis, individualized immuno-/chemotherapeutic strategies and prognosis in patients with LUAD.
Keywords: Lung adenocarcinoma; Metabolism‐related genes; Prognostic; The Cancer Genome Atlas.
Conflict of interest statement
All authors declare no conflict of interests.
Figures







References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
