

Diabetes and Overweight/Obesity Are Independent, Nonadditive Risk Factors for In-Hospital Severity of COVID-19: An International, Multicenter Retrospective Meta-analysis
- PMID: 33858854
- PMCID: PMC8247499
- DOI: 10.2337/dc20-2676
Diabetes and Overweight/Obesity Are Independent, Nonadditive Risk Factors for In-Hospital Severity of COVID-19: An International, Multicenter Retrospective Meta-analysis
Abstract
Objective: Obesity is an established risk factor for severe coronavirus disease 2019 (COVID-19), but the contribution of overweight and/or diabetes remains unclear. In a multicenter, international study, we investigated if overweight, obesity, and diabetes were independently associated with COVID-19 severity and whether the BMI-associated risk was increased among those with diabetes.
Research design and methods: We retrospectively extracted data from health care records and regional databases of hospitalized adult patients with COVID-19 from 18 sites in 11 countries. We used standardized definitions and analyses to generate site-specific estimates, modeling the odds of each outcome (supplemental oxygen/noninvasive ventilatory support, invasive mechanical ventilatory support, and in-hospital mortality) by BMI category (reference, overweight, obese), adjusting for age, sex, and prespecified comorbidities. Subgroup analysis was performed on patients with preexisting diabetes. Site-specific estimates were combined in a meta-analysis.
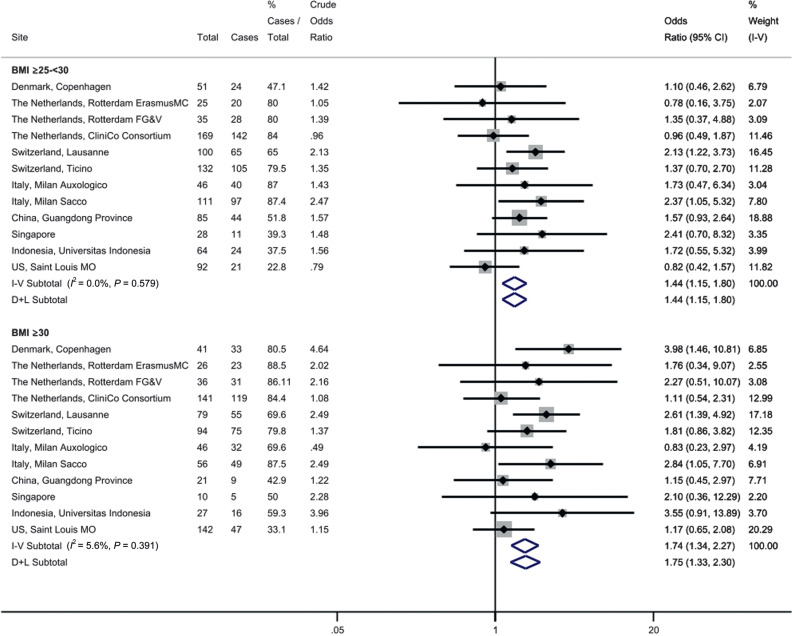
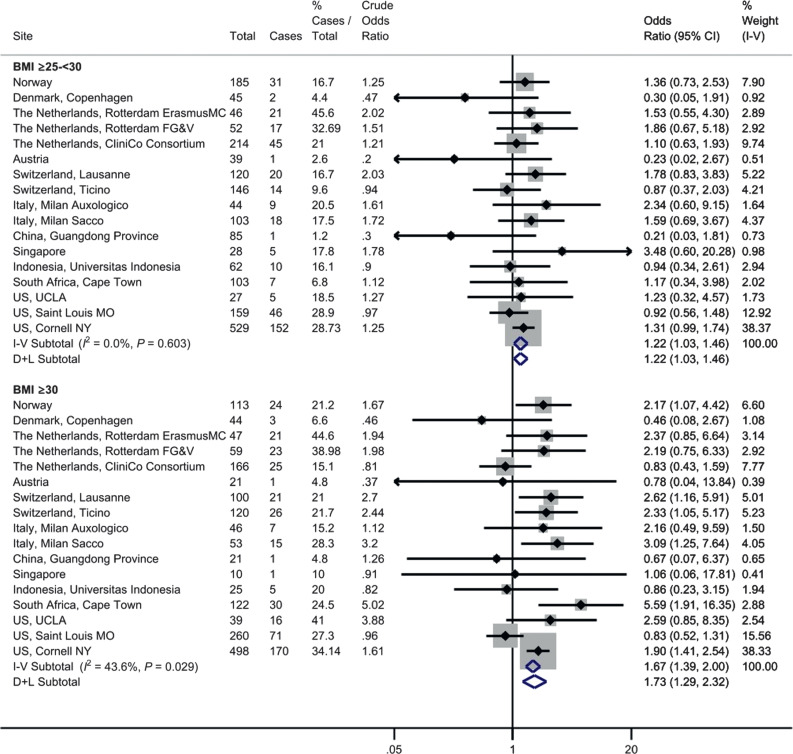
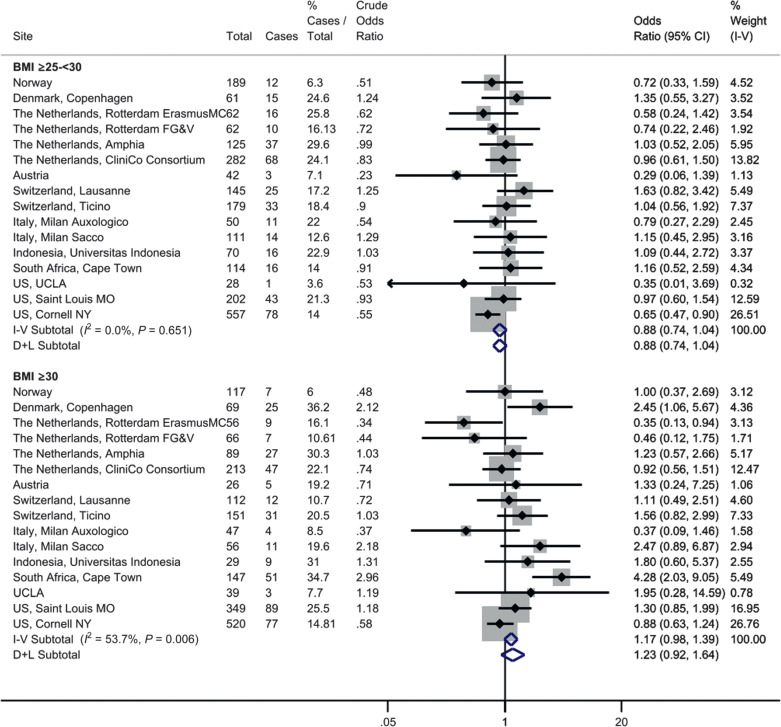
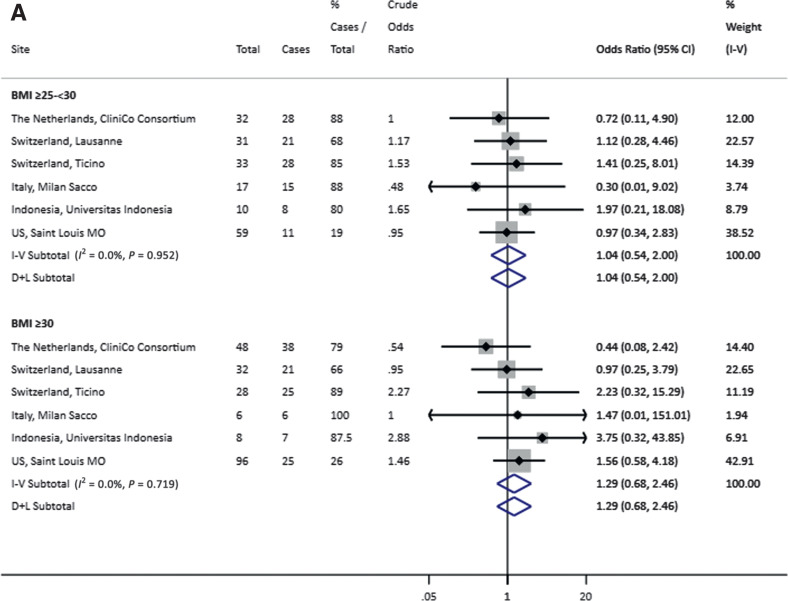
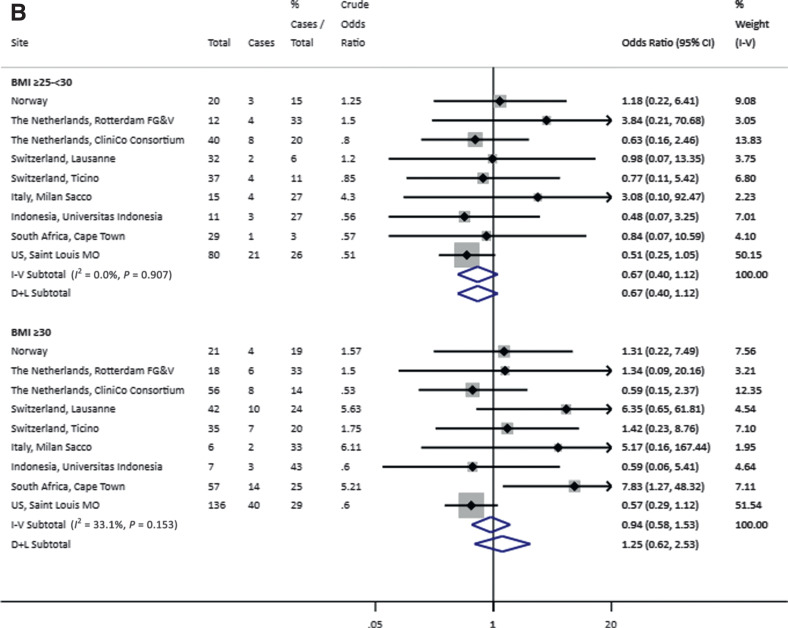
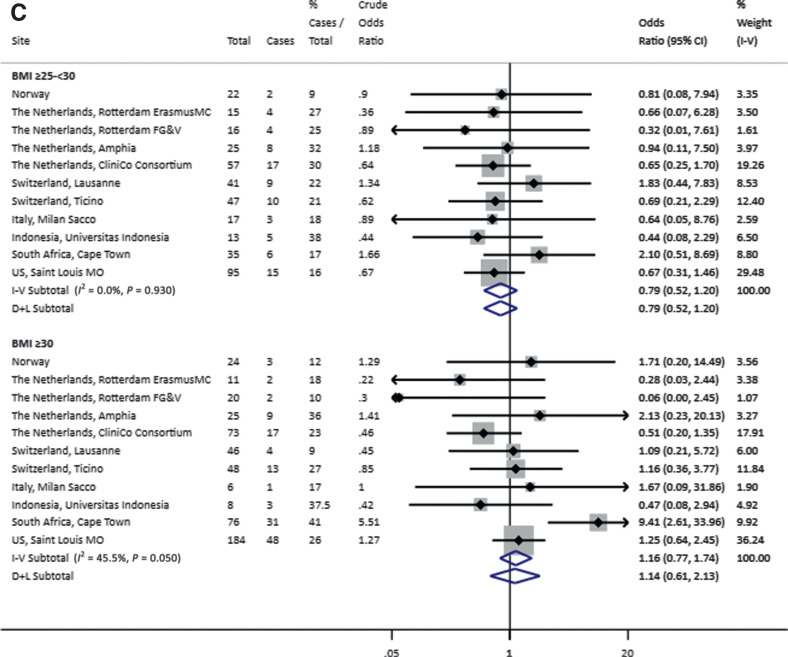
Results: Among 7,244 patients (65.6% overweight/obese), those with overweight were more likely to require oxygen/noninvasive ventilatory support (random effects adjusted odds ratio [aOR], 1.44; 95% CI 1.15-1.80) and invasive mechanical ventilatory support (aOR, 1.22; 95% CI 1.03-1.46). There was no association between overweight and in-hospital mortality (aOR, 0.88; 95% CI 0.74-1.04). Similar effects were observed in patients with obesity or diabetes. In the subgroup analysis, the aOR for any outcome was not additionally increased in those with diabetes and overweight or obesity.
Conclusions: In adults hospitalized with COVID-19, overweight, obesity, and diabetes were associated with increased odds of requiring respiratory support but were not associated with death. In patients with diabetes, the odds of severe COVID-19 were not increased above the BMI-associated risk.
© 2021 by the American Diabetes Association.
Figures
References
-
- World Health Organization . Coronovirus Disease (COVID-19) Situation Report -162. Geneva, World Health Organization, 2020, p. 17
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
