

Erosive Lichen Sclerosus-A Clinicopathologic Subtype
- PMID: 33859124
- PMCID: PMC8231666
- DOI: 10.1097/LGT.0000000000000607
Erosive Lichen Sclerosus-A Clinicopathologic Subtype
Abstract
Objective: The aim of the study was to identify whether erosive lichen sclerosus (LS) is a distinct clinicopathologic subtype.
Materials and methods: The pathology database was searched for "erosion," "erosive," "ulcer," and "lichen sclerosus." Inclusion criteria were histopathologic diagnosis of LS and erosion or ulcer overlying a band of hyalinization and/or fibrosis. Exclusions were concurrent neoplasia and insufficient tissue. Histopathologic review documented site, epithelial thickness, adjacent epidermal characteristics, infiltrate, and dermal collagen abnormality. Clinical data included demographics, comorbidities, examination findings, microbiologic results, treatment, and response.
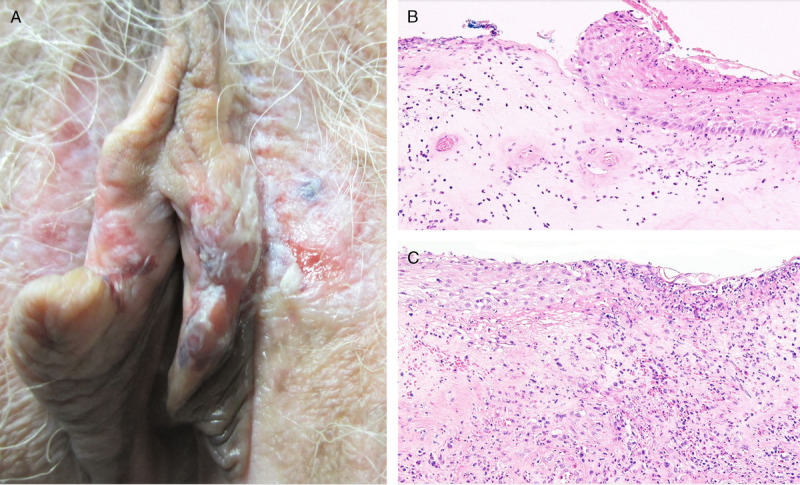
Results: Ten examples of erosive LS and 15 of ulcerated LS occurred in 24 women with a mean age of 67 years. Ulcerated LS was associated with diabetes and nontreatment at time of biopsy. Clinicians identified red patches in all but 1 case of erosive LS. Ulcerated LS was documented as fissure, ulcer, or white plaque, with 8 (53%) described as lichenified LS with epidermal breaches. Erosive LS favored hairless skin with normal adjacent stratum corneum sloping gently into erosion, whereas most ulcers in LS had an abrupt slope from hair-bearing skin. All cases were treated with topical steroids; 2 patients with erosive LS and 10 with ulcerated LS also had oral antifungals, topical estrogen, antibiotics, and/or lesional excision. Treatment yielded complete resolution in 50%.
Conclusions: Erosive LS is an unusual clinicopathologic subtype characterized by red patches on hairless skin seen microscopically as eroded epithelium overlying a band of hyalinized or fibrotic collagen. In contrast, ulcerated LS is usually a traumatic secondary effect in an uncontrolled dermatosis.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the ASCCP.
Conflict of interest statement
The authors have declared they have no conflicts of interest.
Figures



References
-
- Terlou A Santegoets LA van der Meijden WI, et al. . An autoimmune phenotype in vulvar lichen sclerosus and lichen planus: a Th1 response and high levels of microRNA-155. J Invest Dermatol 2012;132:658–66. - PubMed
-
- Lee A, Bradford J, Fischer G. Long-term management of adult vulvar lichen sclerosus: a prospective cohort study of 507 women. JAMA Dermatol 2015;15:1061–7. - PubMed
-
- Sheinis M Green N Vieira-Baptista P, et al. . Adult vulvar lichen sclerosus: can experts agree on the assessment of disease severity? J Low Genit Tract Dis 2020;24:295–8. - PubMed
-
- Vano-Galvan S Fernandez-Guarino M Bea-Ardebol S, et al. . Successful treatment of erosive vulvar lichen sclerosus with methylaminolaevulinic acid and laser-mediated photodynamic therapy. J Eur Acad Dermatol Venerol 2009;23:71–2. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
