

HIV clinical stages and lower extremity arterial disease among HIV infected outpatients in Burundi
- PMID: 33859308
- PMCID: PMC8050048
- DOI: 10.1038/s41598-021-87862-z
HIV clinical stages and lower extremity arterial disease among HIV infected outpatients in Burundi
Abstract
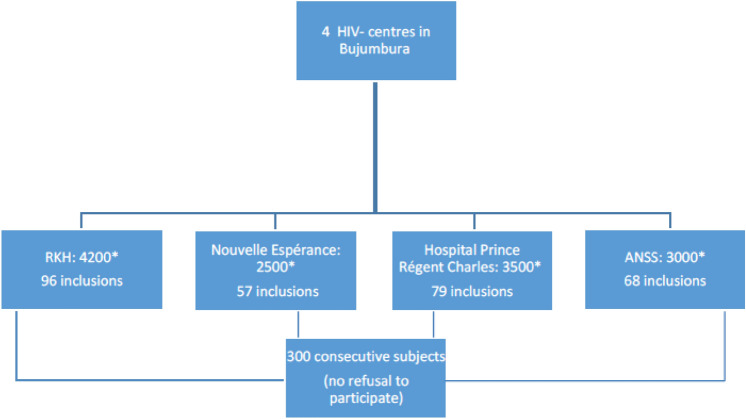
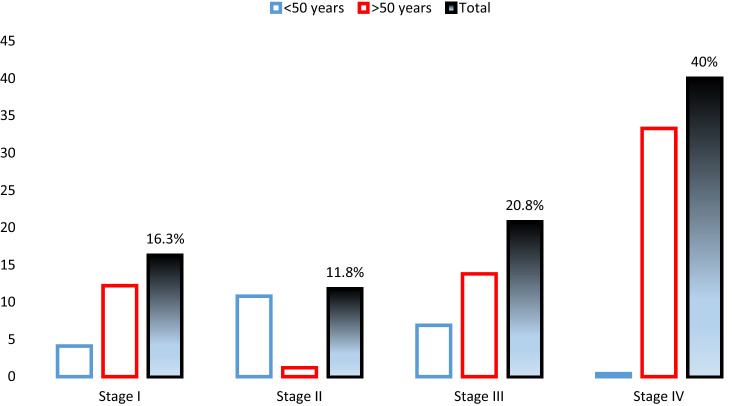
Chronic disease of people living with human immunodeficiency virus (HIV) infection are now approaching those of the general population. Previous, in vitro studies shown that HIV causes arterial injuries resulting in inflammation and atherosclerosis but direct relationship between HIV infection clinical stages and lower extremity arterial disease (LEAD) remain controversial. No study assessed, with an accurate method, both the prevalence of LEAD and the influence of HIV severity on LEAD in HIV outpatients in Central Africa. A cross-sectional study was conducted among 300 HIV-infected outpatients, aged ≥ 40 years in Bujumbura, Burundi. All patients underwent ankle-brachial index (ABI) measurement and LEAD was diagnosed by ABI ≤ 0.9. The prevalence of LEAD was 17.3% (CI 95% 13.2-22.1). The mean age was 49.6 ± 7.1 years. On multivariable analysis, factors associated with LEAD were hypertension (OR = 2.42; 95% CI 1.10-5.80), and stage IV HIV clinical infection (OR = 4.92, 95% CI 1.19-20.36). This is the first study performed on a large HIV population in Central Africa, reporting high LEAD prevalence. It underlines the influence of HIV infection on peripheral atherosclerosis at latest clinical stages and the need for LEAD screening in HIV-infected patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
