

Recurvatum of the Knee in Cerebral Palsy: A Review
- PMID: 33859920
- PMCID: PMC8038913
- DOI: 10.7759/cureus.14408
Recurvatum of the Knee in Cerebral Palsy: A Review
Abstract
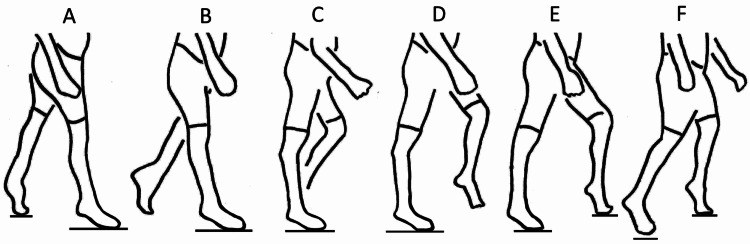
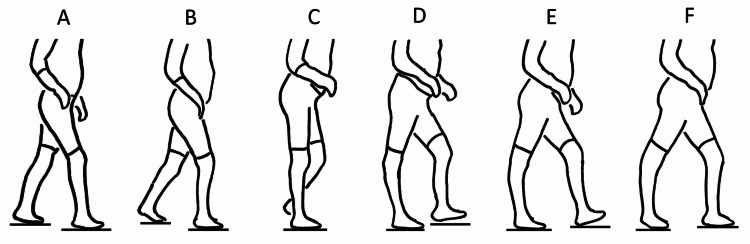
Recurvatum is defined as hyperextension of the knee in the stance phase of gait. Recurvatum knee is a naturally occurring common gait deviation in those with cerebral palsy, along with crouch knee, jump knee, and stiff knee gaits. Early and late recurvatum occur in the first and second halves of stance. Early recurvatum is associated with dynamic calf contraction that raises the heel and pushes the knee into hyperextension as the forefoot contacts the floor. Late recurvatum occurs after the foot is already flat on the floor. As the body weight comes forward over the foot, the tibia stops its forward motion too early as the ankle comes to its range-of-motion limit. The advancing body then moves forward over a hyperextending knee. Surgical hamstring lengthening can have recurvatum as a side effect. There are several strategies to decrease this risk. Medial hamstring lengthening may be safer than combined medial and lateral lengthening. The concept here is that less lengthening or less aggressive lengthening means less recurvatum risk. However, combined medial and lateral lengthening can be reasonably safe from the risk of causing recurvatum if the knee is showing enough preoperative flexion in stance to warrant the increased surgery. More flexion in stance relates to less risk, while less flexion in stance relates to more risk. Knee flexion in stance can be measured. This is done by measuring knee flexion at initial contact and knee flexion in stance in a gait lab or with stop-action video. If there is minimal knee flexion in stance, hamstring lengthening might not be advisable, even if the hamstrings are tight on popliteal angle testing. There are other factors that contribute to recurvatum risk, such as knee hyperextension on static exam, equinus contracture, and jump knee gait. For treatment of recurvatum, the mainstay is the use of ankle foot orthoses set in dorsiflexion. Surgical equinus correction in those with early stance recurvatum can be effective but it is not likely to be effective in those with late stance recurvatum.
Keywords: ankle-foot orthosis; cerebral palsy; gait; hamstring surgery; knee; knee-ankle-foot orthosis; recurvatum; stance.
Copyright © 2021, Yngve et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The efficacy of the floor-reaction ankle-foot orthosis in children with cerebral palsy.J Bone Joint Surg Am. 2009 Oct;91(10):2440-7. doi: 10.2106/JBJS.H.00965. J Bone Joint Surg Am. 2009. PMID: 19797580
-
Ankle and knee coupling in patients with spastic diplegia: effects of gastrocnemius-soleus lengthening.J Bone Joint Surg Am. 2002 May;84(5):736-44. doi: 10.2106/00004623-200205000-00006. J Bone Joint Surg Am. 2002. PMID: 12004014
-
Comparison of hamstring transfer with hamstring lengthening in ambulatory children with cerebral palsy: further follow-up.J Child Orthop. 2014 Dec;8(6):513-20. doi: 10.1007/s11832-014-0626-8. Epub 2014 Nov 28. J Child Orthop. 2014. PMID: 25430874 Free PMC article.
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
The gait and energy efficiency of stance control knee-ankle-foot orthoses: A literature review.Prosthet Orthot Int. 2016 Apr;40(2):202-14. doi: 10.1177/0309364615588346. Epub 2015 Jun 8. Prosthet Orthot Int. 2016. PMID: 26055252 Review.
Cited by
-
Anterior Opening-Wedge High Tibial Osteotomy in the Setting of Genu Recurvatum.Arthrosc Tech. 2023 Oct 2;12(11):e1859-e1866. doi: 10.1016/j.eats.2023.06.007. eCollection 2023 Nov. Arthrosc Tech. 2023. PMID: 38094965 Free PMC article.
-
Control of Tibial Advancement by the Plantar Flexors during the Stance Phase of Gait Depends on Knee Flexion with Respect to the Ground Reaction Force.Bioengineering (Basel). 2023 Dec 31;11(1):41. doi: 10.3390/bioengineering11010041. Bioengineering (Basel). 2023. PMID: 38247918 Free PMC article.
-
Prevalence of congenital anomalies according to maternal race and ethnicity, Texas, 1999-2018.Birth Defects Res. 2024 Jan;116(1):e2274. doi: 10.1002/bdr2.2274. Epub 2023 Nov 28. Birth Defects Res. 2024. PMID: 38014617 Free PMC article.
References
-
- Genu recurvatum in cerebral palsy--part A: influence of dynamic and fixed equinus deformity on the timing of knee recurvatum in children with cerebral palsy. Svehlík M, Zwick EB, Steinwender G, Saraph V, Linhart WE. J Pediatr Orthop B. 2010;19:366–372. - PubMed
-
- Prevalence of genu recurvatum during walking and associated knee pain in chronic hemiplegic stroke patients: a preliminary survey. Tani Y, Otaka Y, Kudo M, Kurayama T, Kondo K. J Stroke Cerebrovasc Dis. 2016;25:1153–1157. - PubMed
-
- The knee and cerebral palsy. Banks HH. Orthop Clin North Am. 1972;3:113–129. - PubMed
-
- Common gait abnormalities of the knee in cerebral palsy. Sutherland DH, Davids JR. https://journals.lww.com/clinorthop/Abstract/1993/03000/Common_Gait_Abno... Clin Orthop Relat Res. 1993;288:139–147. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous