

Gastrointestinal defect closure using a novel through-the-scope helix tack and suture device compared to endoscopic clips in a survival porcine model (with video)
- PMID: 33860074
- PMCID: PMC8041572
- DOI: 10.1055/a-1370-9256
Gastrointestinal defect closure using a novel through-the-scope helix tack and suture device compared to endoscopic clips in a survival porcine model (with video)
Erratum in
-
Erratum: Gastrointestinal defect closure using a novel through-the-scope helix tack and suture device compared to endoscopic clips in a survival porcine model (with video).Endosc Int Open. 2022 May 4;9(4):C12. doi: 10.1055/a-1834-5697. eCollection 2021 Apr. Endosc Int Open. 2022. PMID: 35527742 Free PMC article.
Abstract
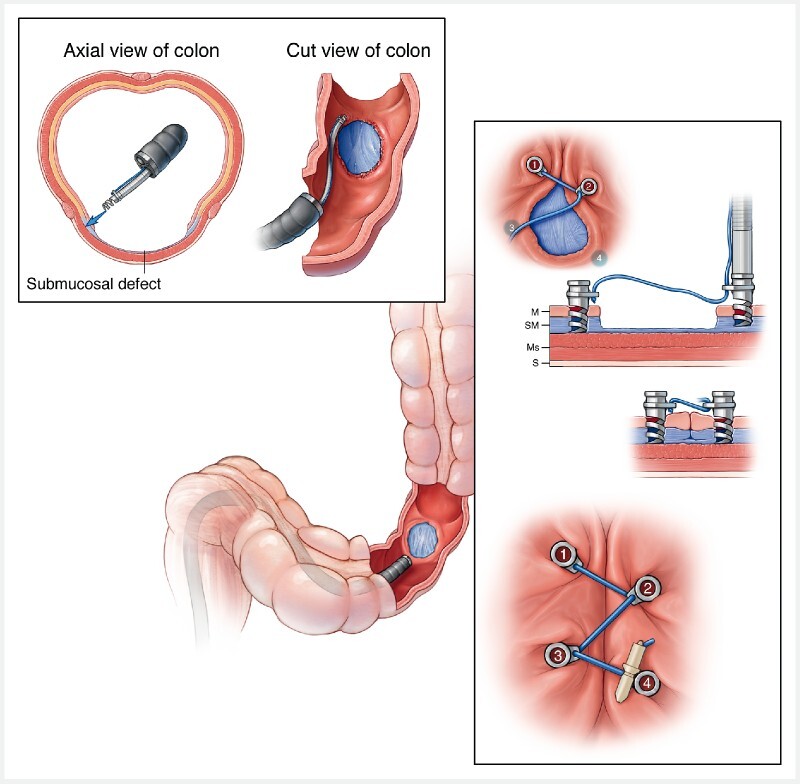
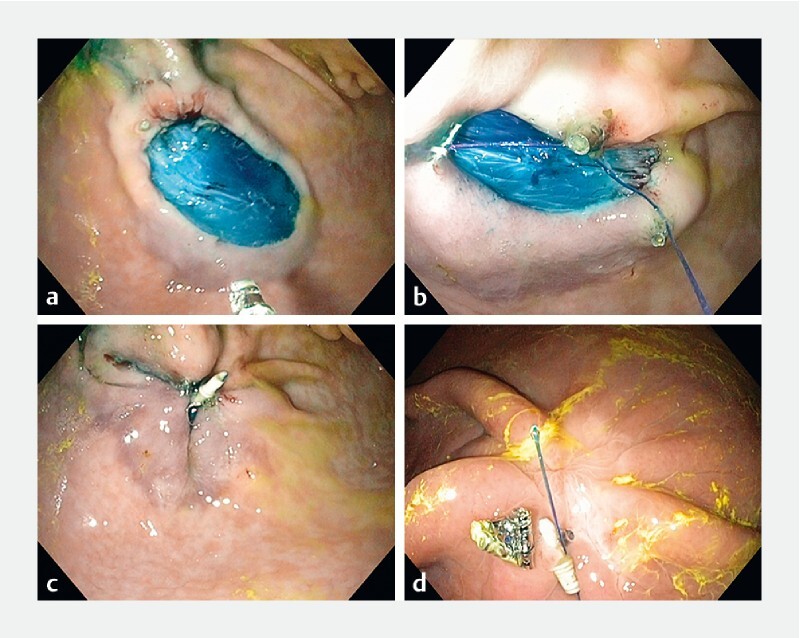
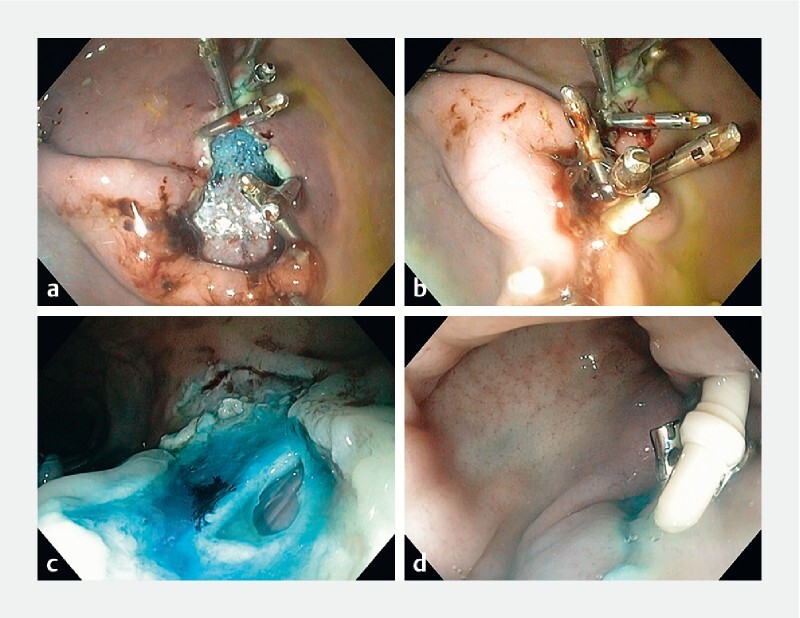
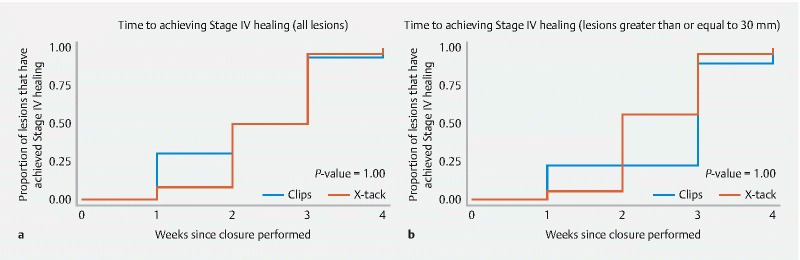
Background and aims Endoscopic resections are associated with bleeding and perforation and may be managed with through-the-scope (TTS) clips, over-the-scope clips and endoscopic suturing. The aim of this preclinical study was to compare technical success of closure using a novel TTS tissue helix tack and suture device (X-Tack) to TTS clips in a porcine model. Materials and methods Four subjects underwent 40 mucosal resections, diameter range 25-50 mm, in the stomach (n = 24) and colon (n = 16). Closures were randomized to X-Tack (n = 24) or clip (n = 16). Animals underwent weekly endoscopic follow-up for 4 weeks. Results Technical closure with X-Tack was successful in 24 of 24 (100 %) cases and with clips in 13 of 16 cases (81.3 %) ( P = 0.0001). One colonic perforation occurred and was successfully managed using X-Tack. The rate of healing was not statistically different between the groups, and all sites healed at 4 weeks including the perforation and were confirmed by histology. Conclusions Compared to TTS clip, X-Tack is superior for effecting large mucosal defect closure, including durable sealing of full-thickness perforation. There was no difference in rate of healing between devices.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests This study was funded by a research grant from Apollo Endosurgery. Dr. Abu Dayyeh has received a research grant from Apollo Endosurgery. Dr. Storm has received a research grant and consulting fees from Apollo Endosurgery and consulting fees from ERBE.
Figures
References
-
- Raju G S. Closure of defects and management of complications. Gastrointest Endosc Clin N Am. 2019;29:705–719. - PubMed
-
- Albeniz E, Alvarez M A, Espinos J C et al. Clip closure after resection of large colorectal lesions with substantial risk of bleeding. Gastroenterology. 2019;157:1213–1.221E7. - PubMed
-
- Sakurai T, Adachi T, Kono M et al. Prophylactic suturing closure is recommended after endoscopic treatment of colorectal tumors in patients with antiplatelet/anticoagulant therapy. Oncology. 2017;93:27–29. - PubMed
-
- Wang Z J, Li S Y, Zhang Y H et al. Endoscopic closure of large colonic perforations with a novel endoscopic clip device: An animal study (with videos) J Gastroenterol Hepatol. 2019;34:2152–2157. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical