

Management of cryptoglandular fistula-in-ano among gastrointestinal surgeons in the Netherlands
- PMID: 33860363
- PMCID: PMC8124037
- DOI: 10.1007/s10151-021-02446-3
Management of cryptoglandular fistula-in-ano among gastrointestinal surgeons in the Netherlands
Abstract
Background: Management of cryptoglandular fistula-in-ano (FIA) can be challenging. Despite Dutch and international guidelines determining optimal therapy is still quite difficult. The aim of this study was to report current practices in the management of cryptoglandular FIA among gastrointestinal surgeons in the Netherlands.
Methods: Dutch surgeons and residents who are treating FIA regularly were sent a survey invitation by email. The survey was available online from September 19 to December 1 2019. The questionnaire consisted of 28 questions concerning diagnostic and surgical techniques in the treatment of intersphincteric and transsphincteric FIA.
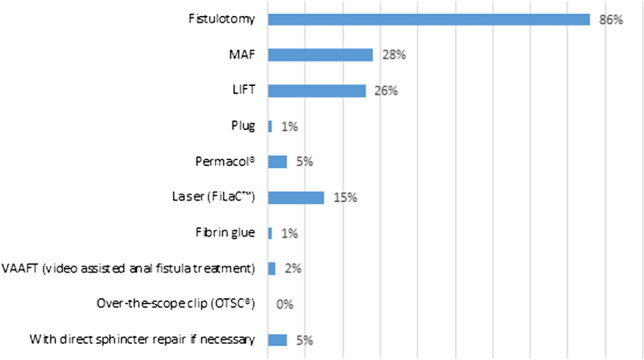
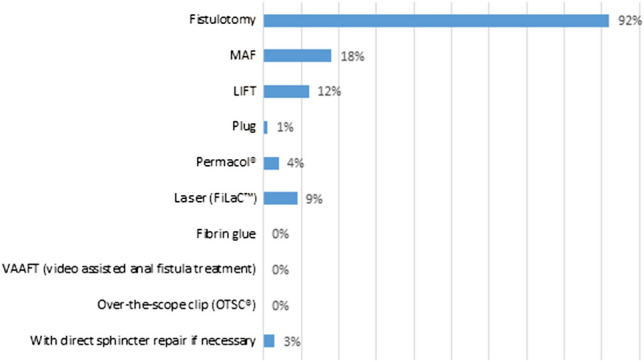
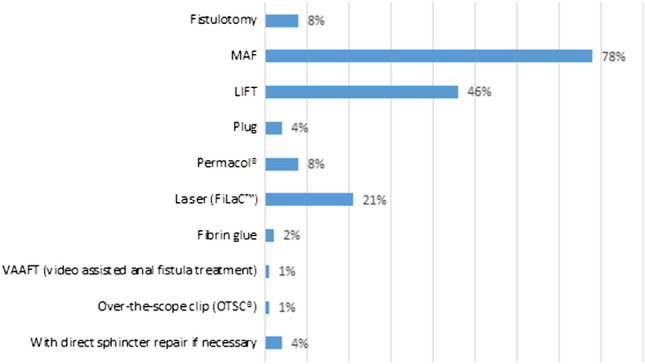
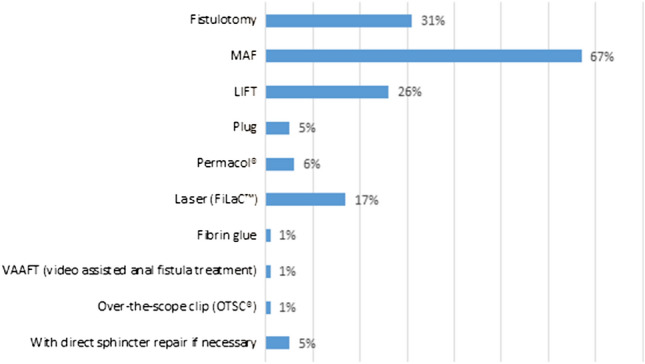
Results: In total, 147 (43%) surgeons responded and completed the survey. Magnetic resonance imaging was the preferred diagnostic imaging modality (97%) followed by the endo-anal ultrasound (12%). In case of a high FIA, 86% used a non-cutting seton. Most respondents removed a seton between 6 weeks and 3 months (n = 84, 58%). Fistulotomy was the procedure of preference in low transsphincteric (86%) and low intersphincteric FIA (92%). Mucosal advancement flap (MAF) and ligation of intersphincteric fistula tract (LIFT), with 78% and 46%, respectively, were the procedures that were applied most often in high transsphincteric FIA. In high intersphincteric FIA 67% performed a MAF and 33% a fistulotomy. Thirty-three percent of all respondents stated that they habitually closed the internal fistula opening, half of them used a Z-plasty. For debridement of the fistula tract the preferred method was curettage (78%).
Conclusions: Dutch gastrointestinal surgeons use various techniques in the management of FIA. Novel promising techniques should be investigated adequately in sufficient large trials to increase consensus. A core outcome measurement and a prospective international database would help in comparing results. Until then, treatment should be adjusted to the individual patient, governed by fistula characteristics and patient choice.
Keywords: Anal fistula; Diagnostic; Fistula in ano; Perianal fistula; Surgical; Survey; Therapy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Corman ML. Classic articles in colon and rectal surgery. Dis Colon Rectum. 1980;23(1):56–59. - PubMed
-
- Vogel JD, et al. Clinical practice guideline for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula. Dis Colon Rectum. 2016;59(12):1117–1133. - PubMed
-
- Ommer A, et al. German S3 guidelines: anal abscess and fistula (second revised version) Langenbeck’s Arch Surg. 2017;402(2):191–201. - PubMed
-
- Chirurgische behandeling van perianale fistels. Richtlijnendatabase 2015. [Online]. Available: https://richtlijnendatabase.nl/richtlijn/proctologie/peri-anale_fistel_e...
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
