

Determining the Electronic Signature of Infection in Electronic Health Record Data
- PMID: 33861547
- PMCID: PMC8217098
- DOI: 10.1097/CCM.0000000000004968
Determining the Electronic Signature of Infection in Electronic Health Record Data
Abstract
Objectives: Recent sepsis studies have defined patients as "infected" using a combination of culture and antibiotic orders rather than billing data. However, the accuracy of these definitions is unclear. We aimed to compare the accuracy of different established criteria for identifying infected patients using detailed chart review.
Design: Retrospective observational study.
Setting: Six hospitals from three health systems in Illinois.
Patients: Adult admissions with blood culture or antibiotic orders, or Angus International Classification of Diseases infection codes and death were eligible for study inclusion as potentially infected patients. Nine-hundred to 1,000 of these admissions were randomly selected from each health system for chart review, and a proportional number of patients who did not meet chart review eligibility criteria were also included and deemed not infected.
Interventions: None.
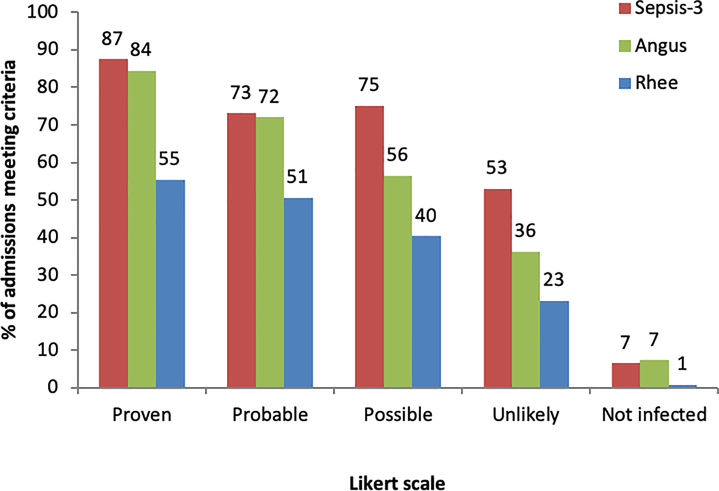
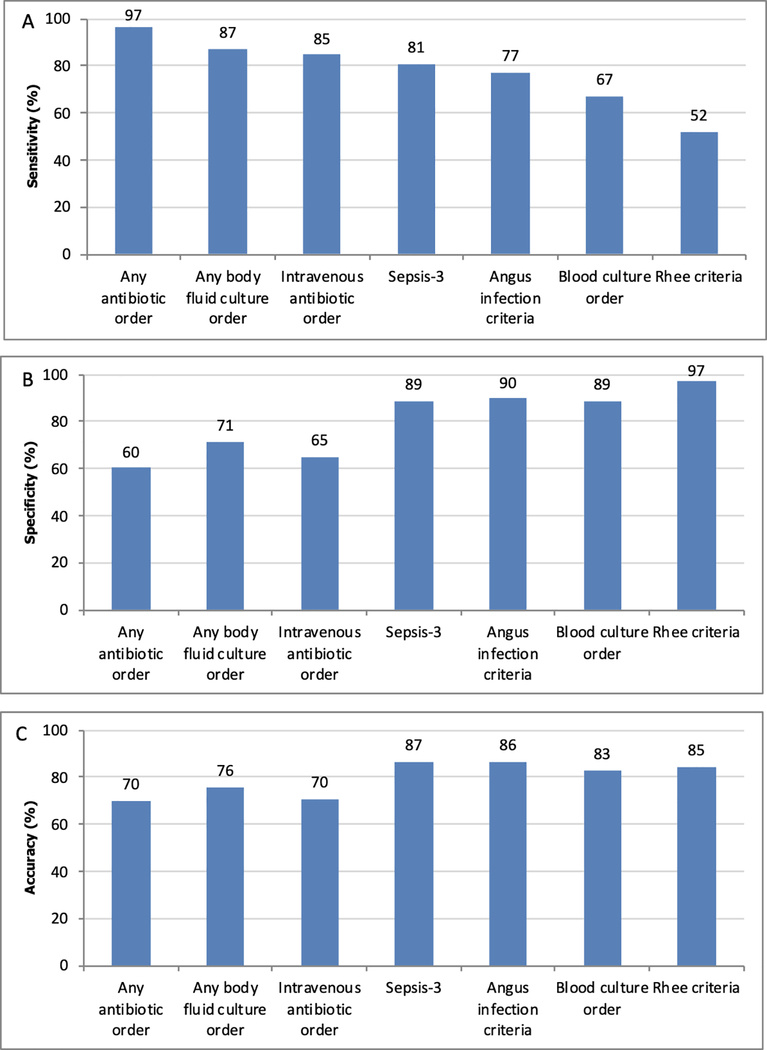
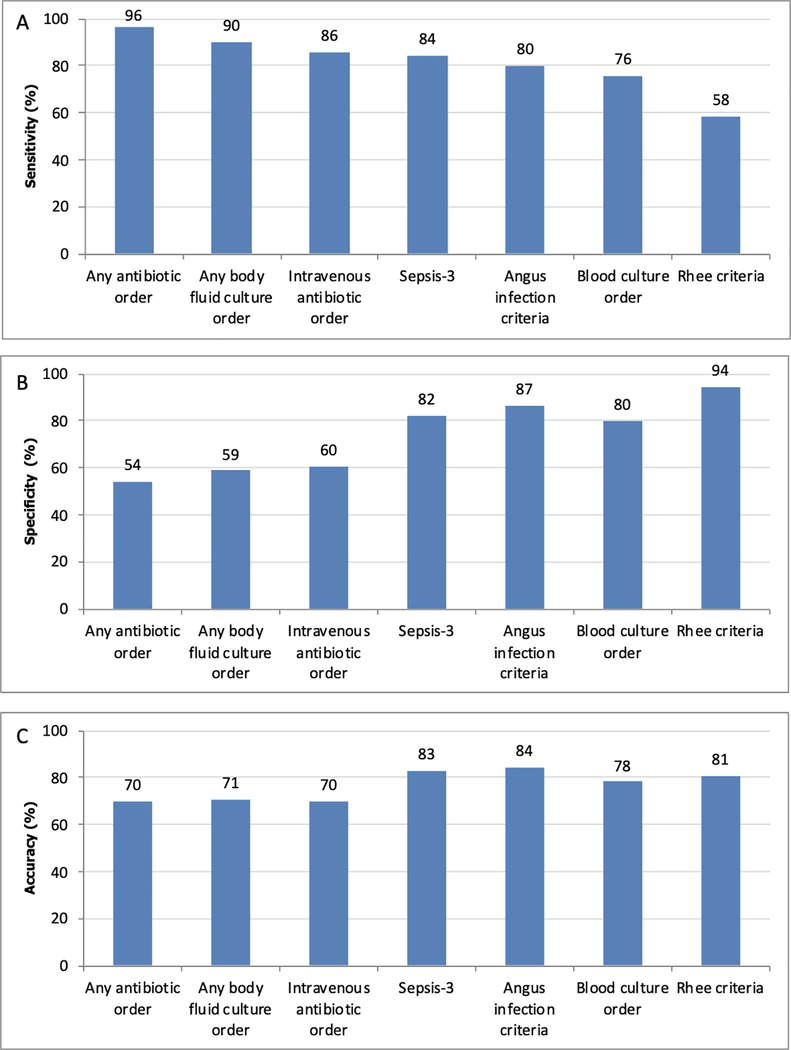
Measurements and main results: The accuracy of published billing code criteria by Angus et al and electronic health record criteria by Rhee et al and Seymour et al (Sepsis-3) was determined using the manual chart review results as the gold standard. A total of 5,215 patients were included, with 2,874 encounters analyzed via chart review and a proportional 2,341 added who did not meet chart review eligibility criteria. In the study cohort, 27.5% of admissions had at least one infection. This was most similar to the percentage of admissions with blood culture orders (26.8%), Angus infection criteria (28.7%), and the Sepsis-3 criteria (30.4%). Sepsis-3 criteria was the most sensitive (81%), followed by Angus (77%) and Rhee (52%), while Rhee (97%) and Angus (90%) were more specific than the Sepsis-3 criteria (89%). Results were similar for patients with organ dysfunction during their admission.
Conclusions: Published criteria have a wide range of accuracy for identifying infected patients, with the Sepsis-3 criteria being the most sensitive and Rhee criteria being the most specific. These findings have important implications for studies investigating the burden of sepsis on a local and national level.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Drs. Churpek and Edelson received funding from National Institute of General Medical Sciences R01 GM123193; disclosed a patent pending (ARCD. P0535US. P2) for risk stratification algorithms for hospitalized patients and have received research support from EarlySense (Tel Aviv, Israel). Drs. Churpek, Winslow, Shah, and Afshar received support for article research from the National Institutes of Health. Dr. Afshar also received support from a K23 from National Institute on Alcohol Abuse and Alcoholism K23 AA024503. Dr. Edelson received support for article research from the American Heart Association (Dallas, TX) and Laerdal Medical (Stavanger, Norway), and she received research support from Philips Healthcare (Andover, MA). She disclosed ownership interest in Quant HC (Chicago, IL), which is developing products for risk stratification of hospitalized patients; she is president/co-founder and shareholder of AgileMD with licensing agreements with Philips Healthcare and EarlySense; and she is the chair for the American Heart Association Get with The Guidelines adult research task force. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, et al.: Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29(7):1303–1310 - PubMed
-
- Liu V, Escobar GJ, Greene JD, Soule J, et al.: Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014; 312(1):90–92 - PubMed
-
- Valles J, Fontanals D, Oliva JC, Martinez M, et al.: Trends in the incidence and mortality of patients with community-acquired septic shock 2003–2016. Journal of critical care 2019; 53:46–52 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
