

Impact of smoke-free ordinance strength on smoking prevalence and lung cancer incidence
- PMID: 33861796
- PMCID: PMC8051804
- DOI: 10.1371/journal.pone.0250285
Impact of smoke-free ordinance strength on smoking prevalence and lung cancer incidence
Abstract
Background: Smoke-free ordinances (SFO) have been shown to be effective public health interventions, but there is limited data on the impact SFO on lung cancer outcomes. We explored the effect of county-level SFO strength with smoking prevalence and lung cancer incidence in Indiana.
Methods: We obtained county-level lung cancer incidence from the Indiana State Cancer Registry and county-level characteristics from the Indiana Tobacco Prevention and Cessation Commission's policy database between 1995 and 2016. Using generalized estimating equations, we performed multivariable analyses of smoking prevalence and age-adjusted lung cancer rates with respect to the strength of smoke-free ordinances at the county level over time.
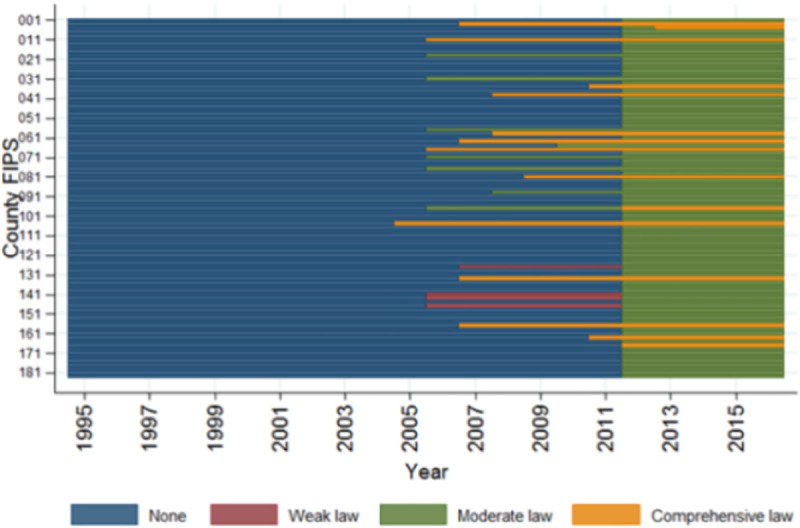
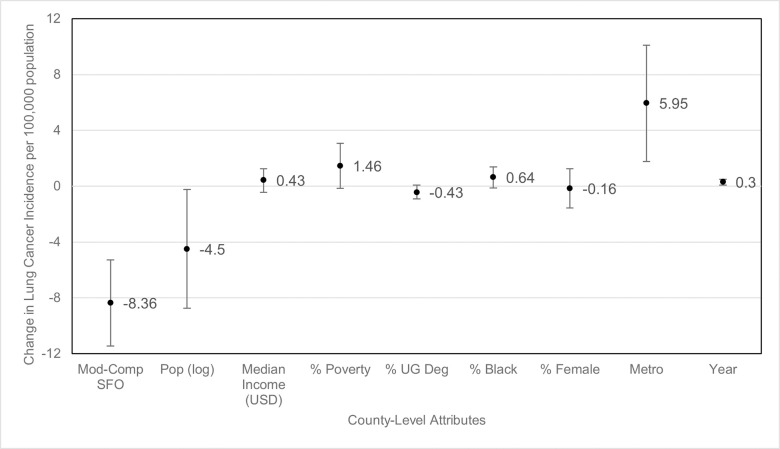
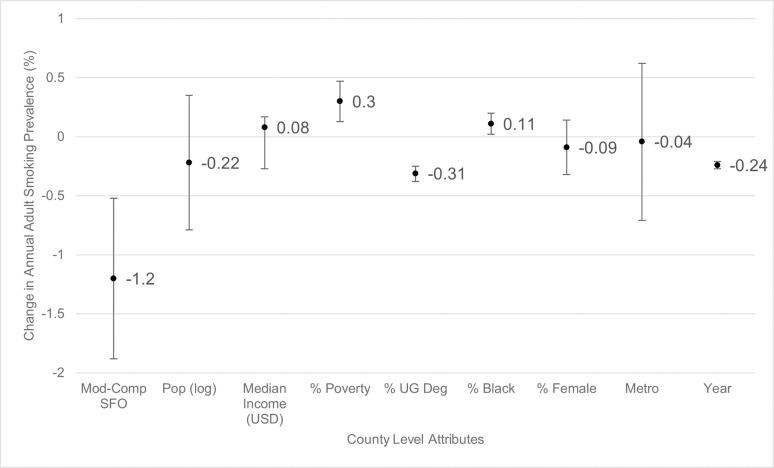
Results: Of Indiana's 92 counties, 24 had a SFO by 2011. In 2012, Indiana enacted a state-wide SFO enforcing at least moderate level SFO protection. Mean age-adjusted lung cancer incidence per year was 76.8 per 100,000 population and mean smoking prevalence per year was 25% during the study period. Counties with comprehensive or moderate SFO had a smoking prevalence 1.2% (95% CI [-1.88, -0.52]) lower compared with counties with weak or no SFO. Counties that had comprehensive or moderate SFO also had an 8.4 (95% CI [-11.5, -5.3]) decrease in new lung cancer diagnosis per 100,000 population per year compared with counties that had weak or no SFO.
Conclusion: Counties with stronger smoke-free air ordinances were associated with decreased smoking prevalence and fewer new lung cancer cases per year. Strengthening SFO is paramount to decreasing lung cancer incidence.
Conflict of interest statement
No authors have competing interests.
Figures
References
-
- National Center for Chronic Disease P, Health Promotion Office on S, Health. Reports of the Surgeon General. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2014.
-
- Centers for Disease Control and Prevention NCfCDPaHP, Division of Population Health. BRFSS Prevalence & Trends Data. 2015.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
