

Social cognition in 22q11.2 deletion syndrome and idiopathic developmental neuropsychiatric disorders
- PMID: 33863277
- PMCID: PMC8052741
- DOI: 10.1186/s11689-021-09363-4
Social cognition in 22q11.2 deletion syndrome and idiopathic developmental neuropsychiatric disorders
Abstract
Background: 22q11.2 deletion syndrome (22q11DS) is a common recurrent neurogenetic condition associated with elevated risk for developmental neuropsychiatric disorders and intellectual disability. Children and adults with 22q11DS often exhibit marked social impairment as well as neurocognitive deficits, and have elevated rates of both autism spectrum disorder (ASD) and psychosis. However, the relationship between the basic processes of social cognition and cognitive ability has not been well studied in 22q11DS. Here, we examined differences in social cognition in 22q11DS, relative to multiple groups of idiopathic neuropsychiatric disorders, and typically developing healthy controls (HC). Additionally, we examined differences in intellectual functioning and its relationship to social cognitive abilities. Finally, we examined the relationship between social cognitive abilities and real-world social behavior.
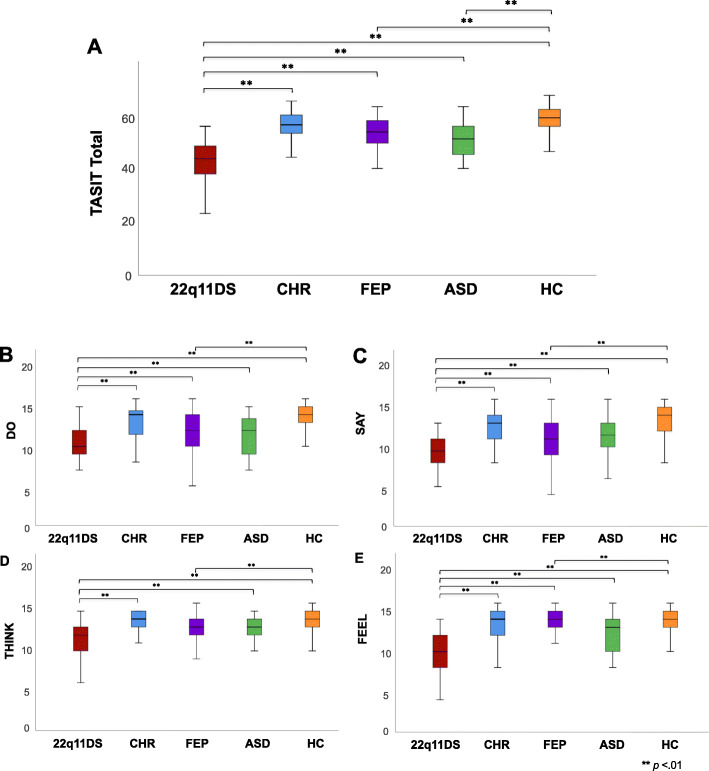
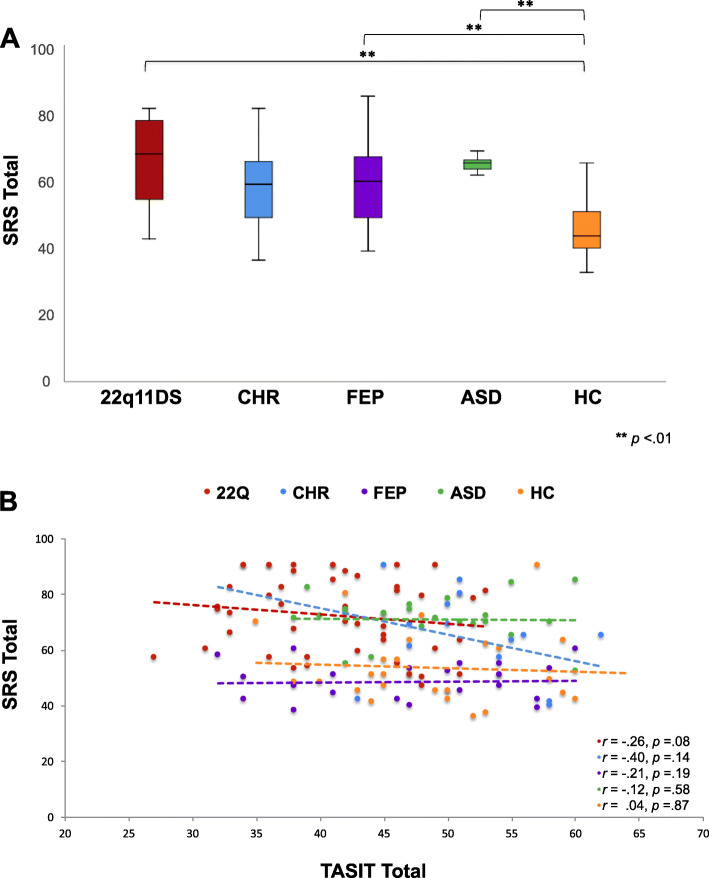
Methods: We examined social cognition and intellectual functioning in 273 participants (mean age = 17.74 ± 5.18% female = 44.3%): 50 with 22q11DS, 49 youth with first episode psychosis (FEP), 48 at clinical high-risk (CHR) for psychosis, 24 participants with ASD, and 102 HC. Social cognition was assessed using The Awareness of Social Inference Test (TASIT), while reciprocal social behavior was assessed via parent/caregiver ratings on the Social Responsiveness Scale (SRS). Participants were also administered the Wechsler Abbreviated Scale of Intelligence, 2nd edition (WASI-II) to assess intellectual functioning.
Results: The 22q11DS group exhibited significantly lower social cognitive abilities compared to CHR, FEP, and HC groups after controlling for intellectual functioning, but not in comparison to the ASD group. Significant positive correlations were found between social cognition, as measured by the TASIT and IQ across groups. In contrast, no significant relationships were found between TASIT and real-world social behavior (SRS) for any group.
Conclusions: Our findings indicate social cognitive deficits are more prominent in 22q11DS than idiopathic neuropsychiatric conditions across the age range, even after adjusting for global intellectual function. These results contribute to our understanding of the intellectual and social vulnerabilities of 22q11DS in comparison to idiopathic neuropsychiatric disorders. Our findings of robust associations between intellectual ability and social cognition emphasizes the importance of accounting for neurocognitive deficits in social skills interventions and tailoring these existing treatment models for 22q11DS and other populations with intellectual impairment.
Keywords: 22q11.2 deletion; Autism spectrum disorder; Neurocognition; Psychosis; Social cognition.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Goldenberg PC, Calkins ME, Richard J, McDonald-McGinn D, Zackai E, Mitra N, Emanuel B, Devoto M, Borgmann-Winter K, Kohler C, Conroy CG, Gur RC, Gur RE. Computerized neurocognitive profile in young people with 22q11.2 deletion syndrome compared to youths with schizophrenia and at-risk for psychosis. Am J Med Genet B Neuropsychiatr Genet. 2012;159B(1):87–93. doi: 10.1002/ajmg.b.32005. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
