

Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: a systematic review and meta-analysis
- PMID: 33863345
- PMCID: PMC8052671
- DOI: 10.1186/s12984-021-00857-9
Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: a systematic review and meta-analysis
Abstract
Background: Robotic-Assisted Gait Training (RAGT) may enable high-intensive and task-specific gait training post-stroke. The effect of RAGT on gait movement patterns has however not been comprehensively reviewed. The purpose of this review was to summarize the evidence for potentially superior effects of RAGT on biomechanical measures of gait post-stroke when compared with non-robotic gait training alone.
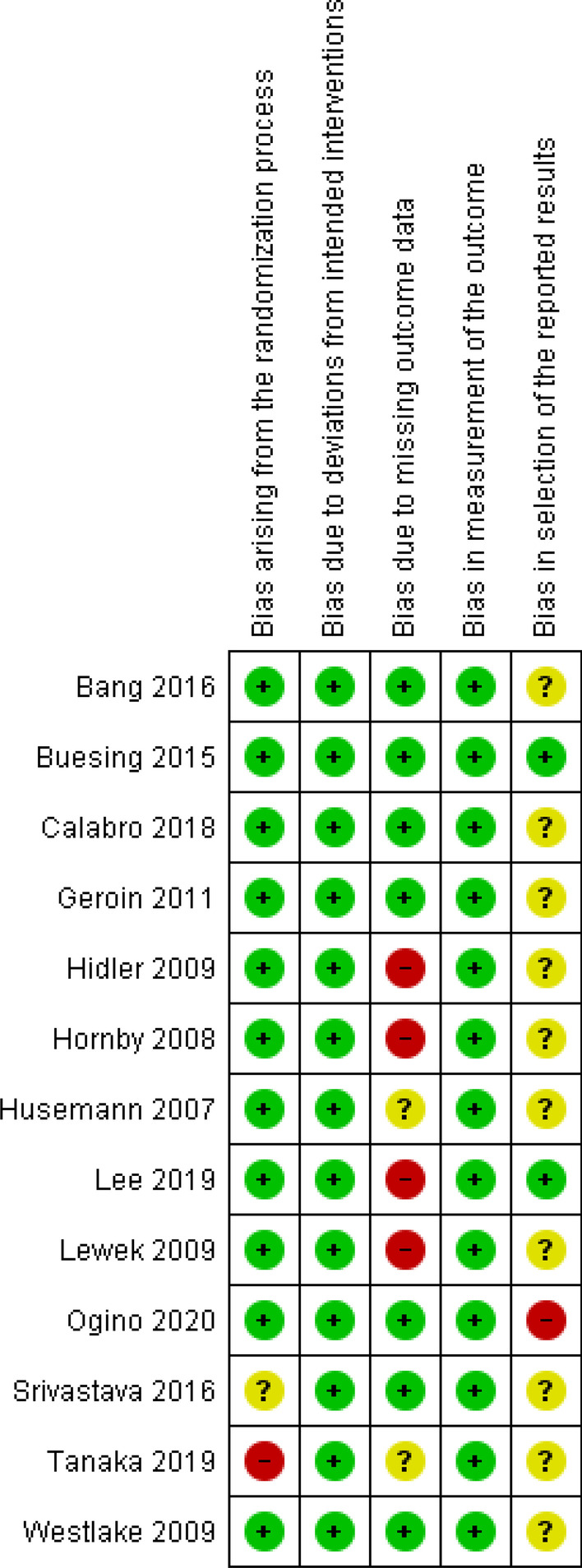
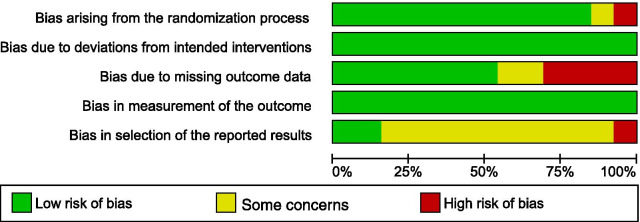
Methods: Nine databases were searched using database-specific search terms from their inception until January 2021. We included randomized controlled trials investigating the effects of RAGT (e.g., using exoskeletons or end-effectors) on spatiotemporal, kinematic and kinetic parameters among adults suffering from any stage of stroke. Screening, data extraction and judgement of risk of bias (using the Cochrane Risk of bias 2 tool) were performed by 2-3 independent reviewers. The Grading of Recommendations Assessment Development and Evaluation (GRADE) criteria were used to evaluate the certainty of evidence for the biomechanical gait measures of interest.
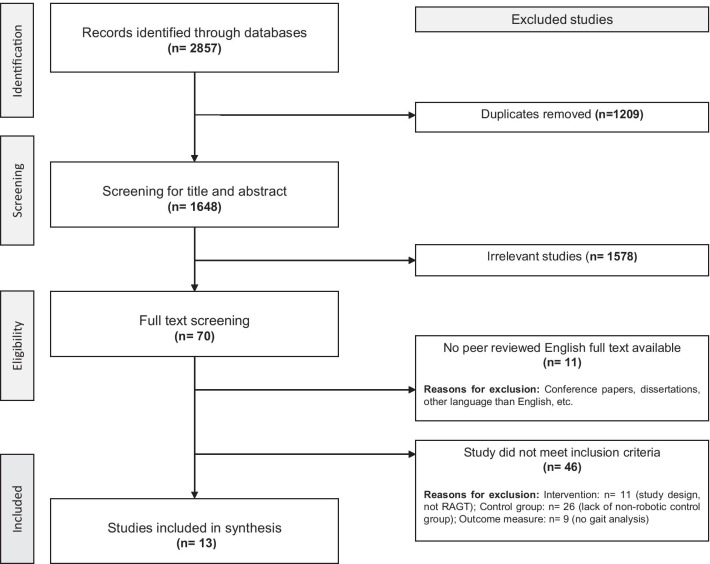
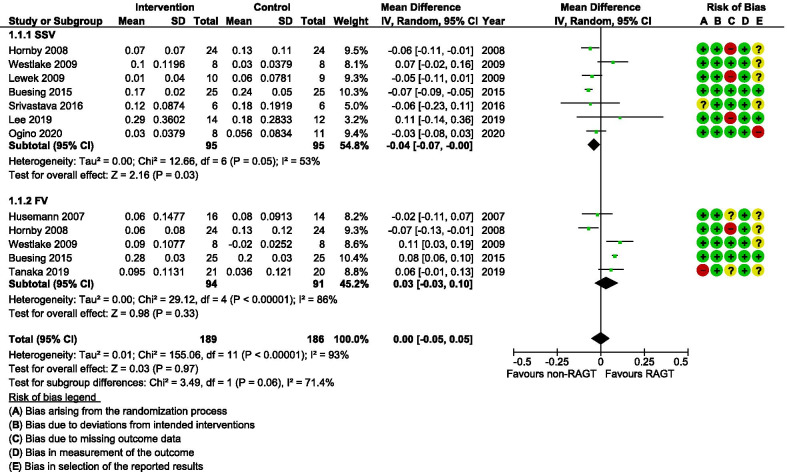
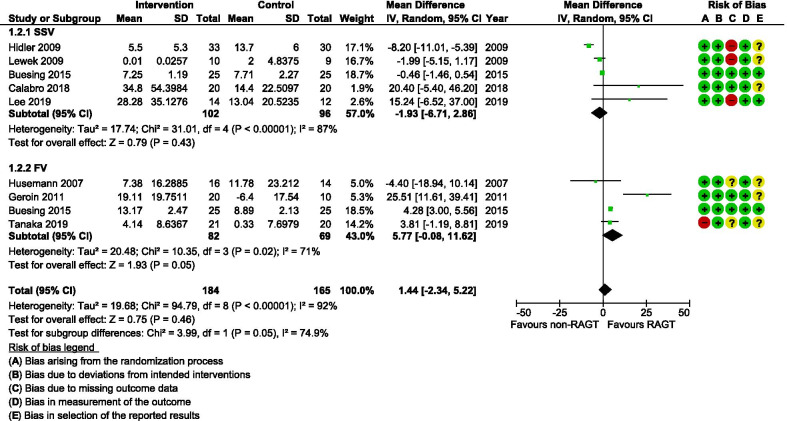
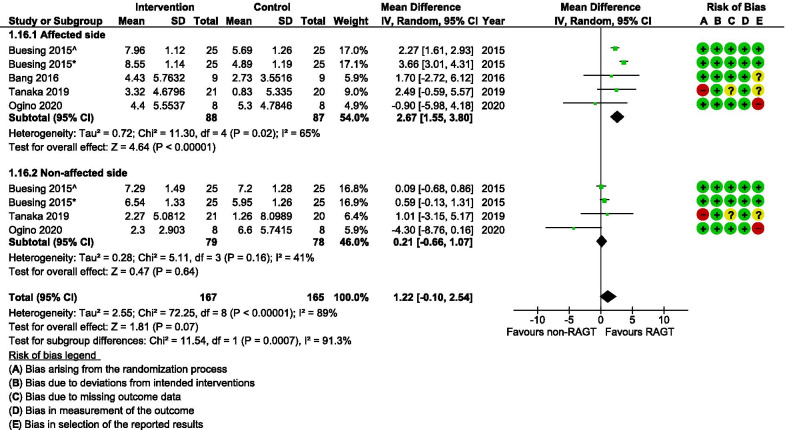
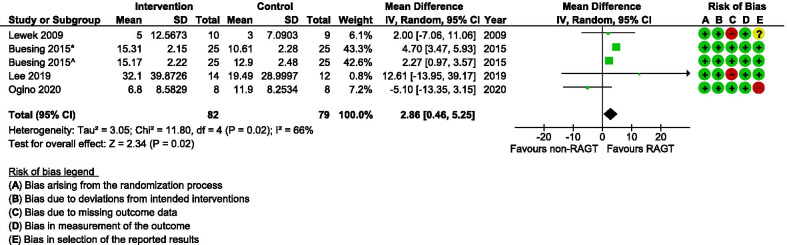
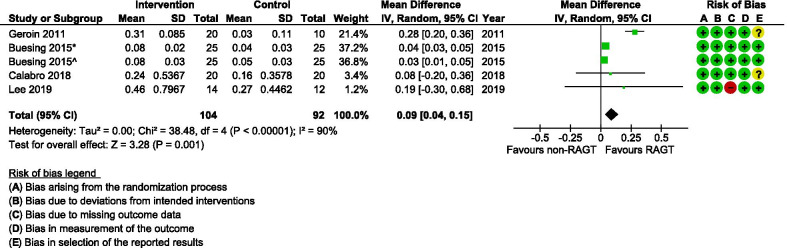
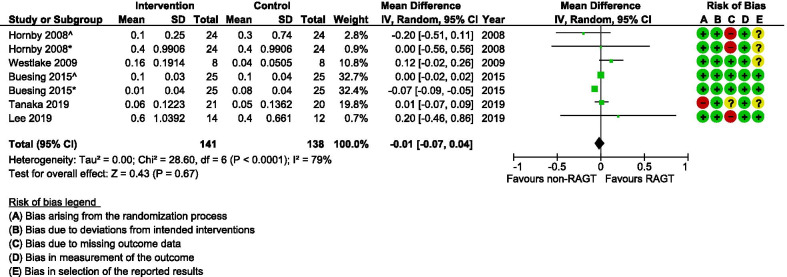
Results: Thirteen studies including a total of 412 individuals (mean age: 52-69 years; 264 males) met eligibility criteria and were included. RAGT was employed either as monotherapy or in combination with other therapies in a subacute or chronic phase post-stroke. The included studies showed a high risk of bias (n = 6), some concerns (n = 6) or a low risk of bias (n = 1). Meta-analyses using a random-effects model for gait speed, cadence, step length (non-affected side) and spatial asymmetry revealed no significant differences between the RAGT and comparator groups, while stride length (mean difference [MD] 2.86 cm), step length (affected side; MD 2.67 cm) and temporal asymmetry calculated in ratio-values (MD 0.09) improved slightly more in the RAGT groups. There were serious weaknesses with almost all GRADE domains (risk of bias, consistency, directness, or precision of the findings) for the included outcome measures (spatiotemporal and kinematic gait parameters). Kinetic parameters were not reported at all.
Conclusion: There were few relevant studies and the review synthesis revealed a very low certainty in current evidence for employing RAGT to improve gait biomechanics post-stroke. Further high-quality, robust clinical trials on RAGT that complement clinical data with biomechanical data are thus warranted to disentangle the potential effects of such interventions on gait biomechanics post-stroke.
Keywords: Cerebrovascular accident; Literature synthesis; Powered exoskeleton; Rehabilitation; Walk.
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Lefeber N, Swinnen E, Kerckhofs E. The immediate effects of robot-assistance on energy consumption and cardiorespiratory load during walking compared to walking without robot-assistance: a systematic review. Disabil Rehabil Assist Technol. 2017;12:657–671. doi: 10.1080/17483107.2016.1235620. - DOI - PubMed
-
- Goffredo M, Guanziroli E, Pournajaf S, Gaffuri M, Gasperini G, Filoni S, et al. Overground wearable powered exoskeleton for gait training in subacute stroke subjects: clinical and gait assessments. Eur J Phys Rehabil Med. 2019;55:710–721. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
