

Intra-patient comparison of physiologic 68Ga-PSMA-11 and 18F-DCFPyL PET/CT uptake in ganglia in prostate cancer patients: a pictorial essay
- PMID: 33863390
- PMCID: PMC8052677
- DOI: 10.1186/s40644-021-00404-8
Intra-patient comparison of physiologic 68Ga-PSMA-11 and 18F-DCFPyL PET/CT uptake in ganglia in prostate cancer patients: a pictorial essay
Abstract
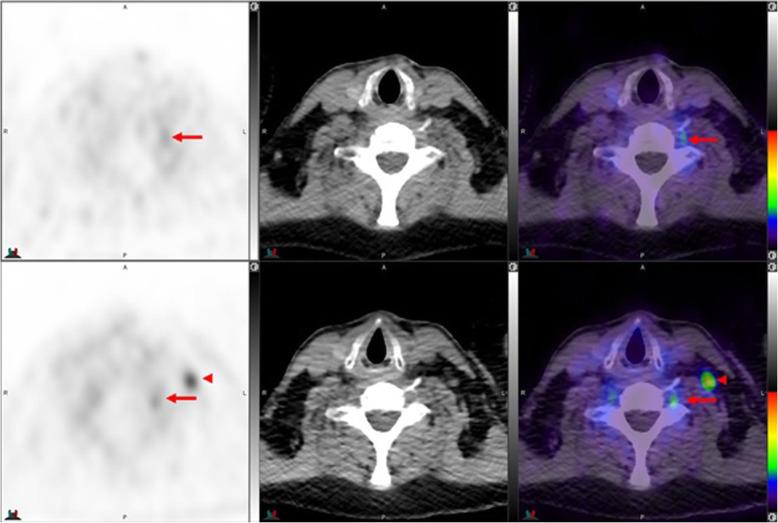
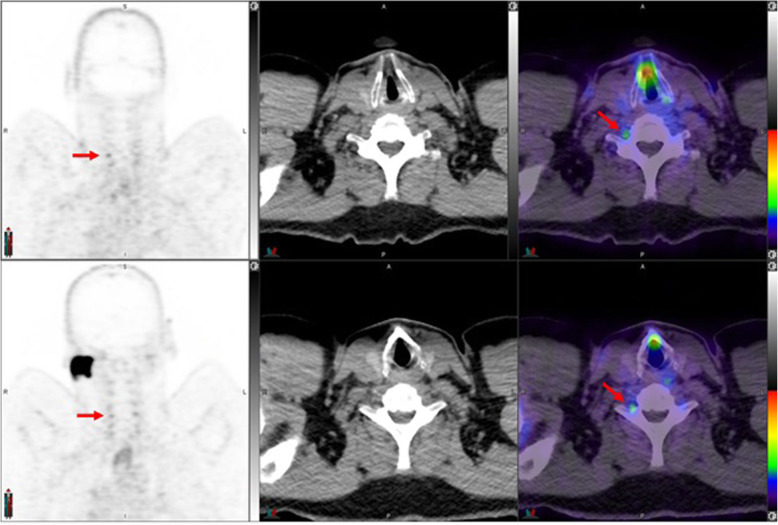
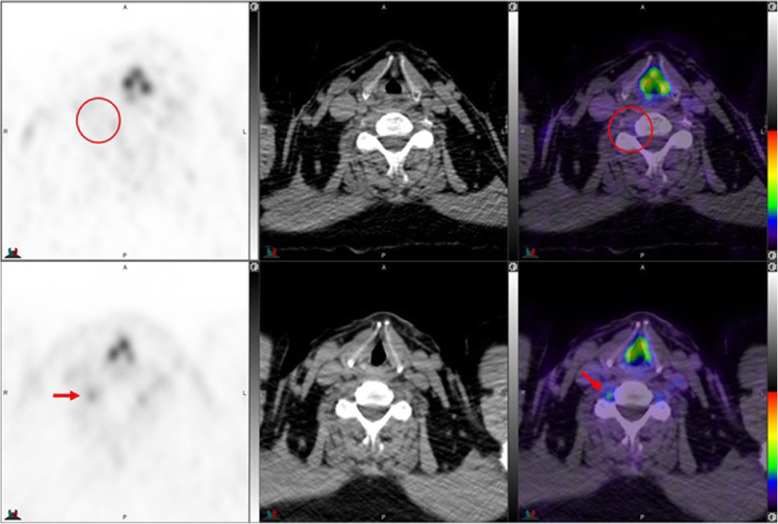
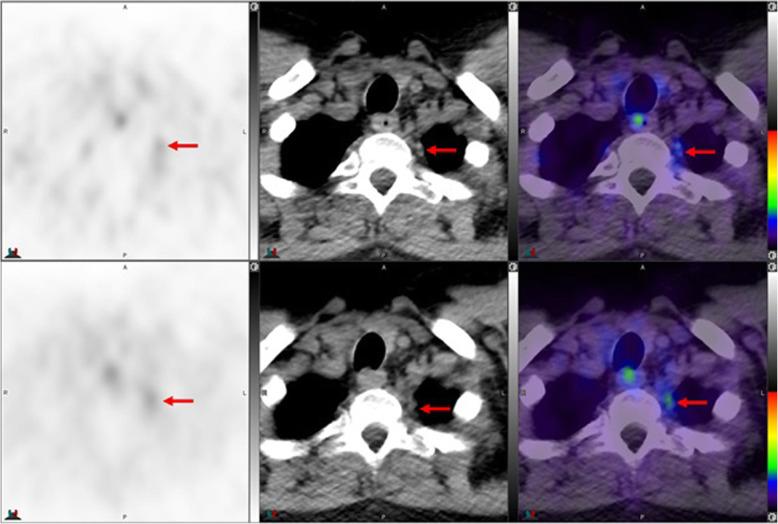
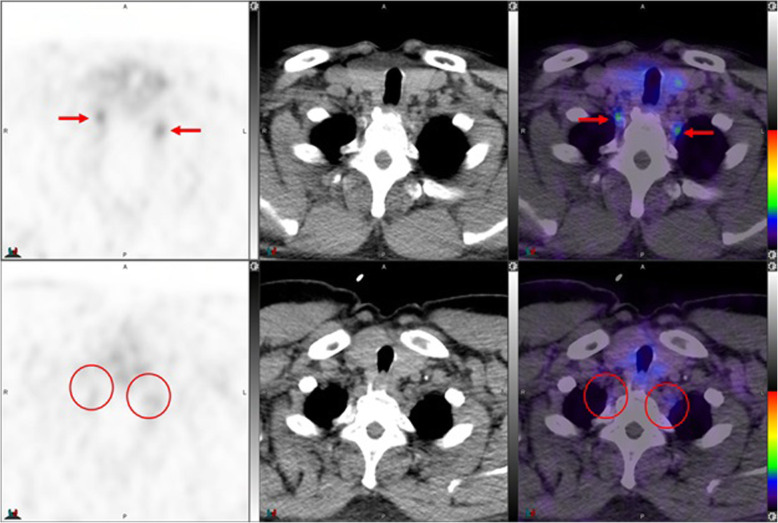
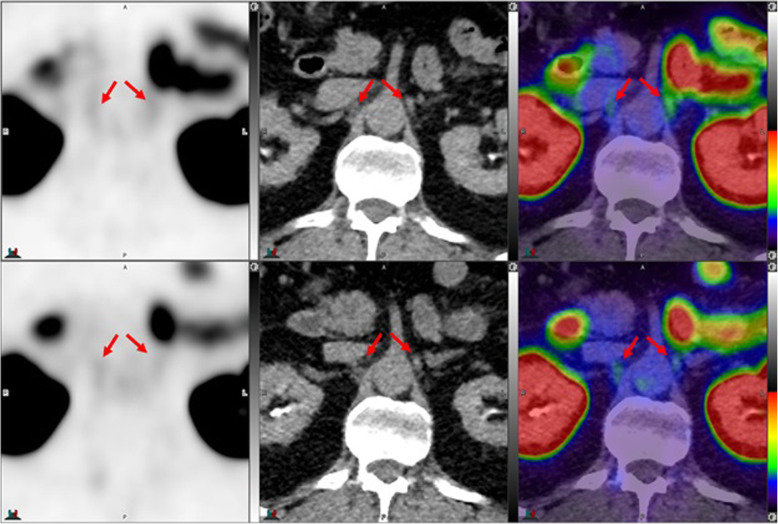
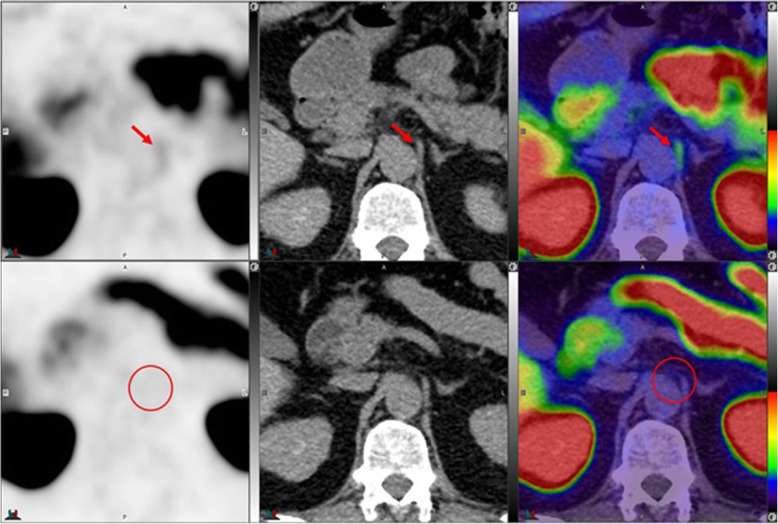
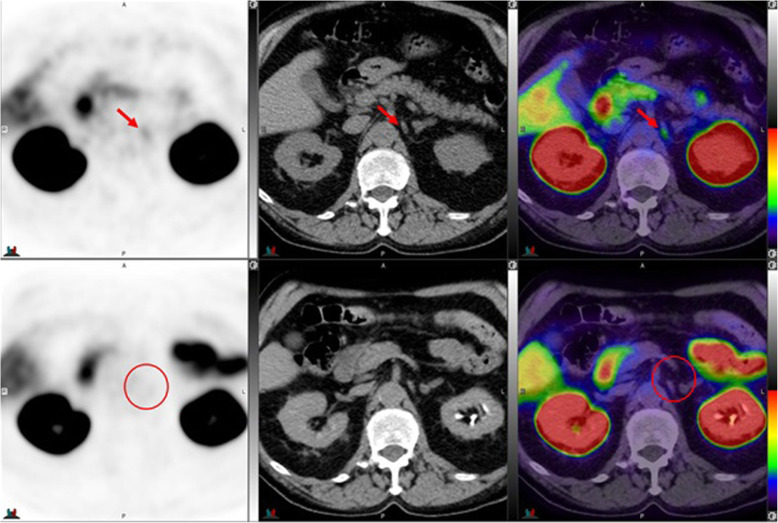
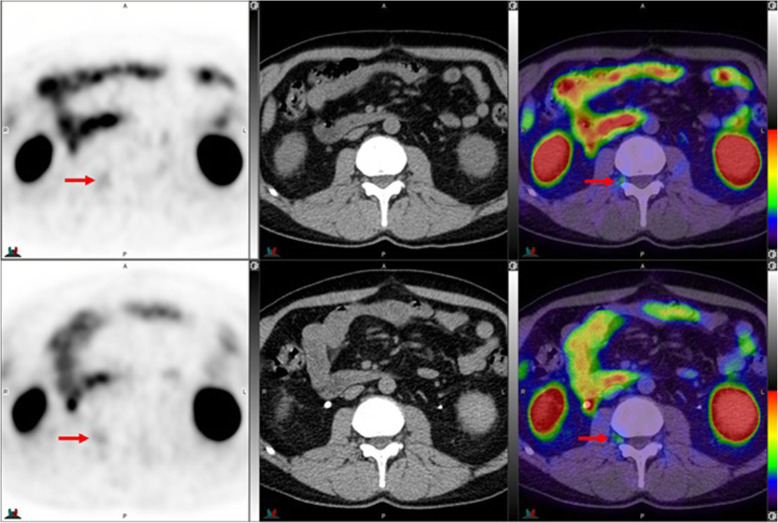
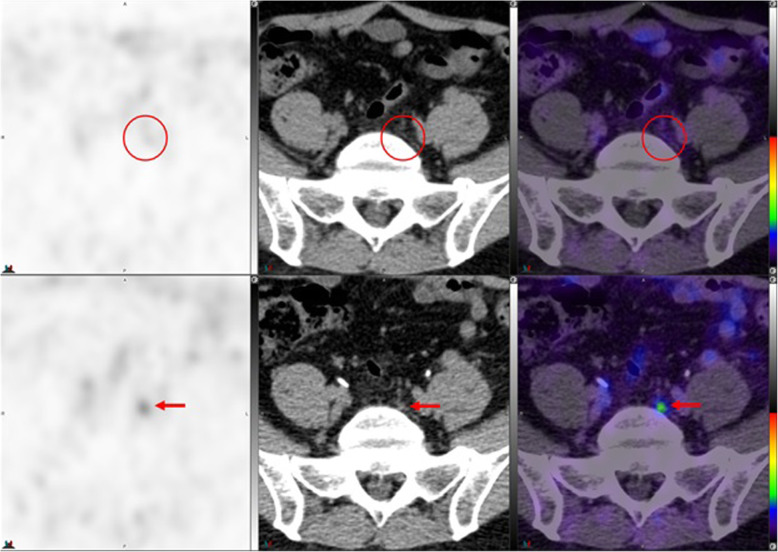
Background: Recent studies reported metabolic uptake in at least one of the evaluated ganglia in 98.5% of patients undergoing 68Ga -PSMA-11 and in 96.9% of patients undergoing 18F-DCFPyL PET/CT examination. We have observed different patterns of ganglion visualization with 18F-DCFPyL compared to 68Ga-PSMA-11. This includes more frequent visualization of cervical and sacral ganglia, which may be attributable to better imaging characteristics with 18F PET imaging.
Case presentation: This pictorial essay is to illustrate and compare, in the same patient, various representative cases of 68Ga-PSMA-11 and 18F-DCFPyL PET/CT uptake in ganglia at different anatomic locations, with different patterns and distribution of metabolic activity.
Conclusion: Reading physicians should be aware of the frequently encountered and occasionally different physiologic uptake of 68Ga-PSMA-11 and 18F DCFPyL in different ganglia.
Keywords: 18F-DCFPyL PET/CT; 68Ga-PSMA11 PET/CT; Ganglia; PSMA.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, Rutherford N, Martin JM, Frydenberg M, Shakher R, Wong LM, Taubman K, Ting Lee S, Hsiao E, Roach P, Nottage M, Kirkwood I, Hayne D, Link E, Marusic P, Matera A, Herschtal A, Iravani A, Hicks RJ, Williams S, Murphy DG. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet. 2020;395(10231):1208–1216. doi: 10.1016/S0140-6736(20)30314-7. - DOI - PubMed
-
- Eiber M, Maurer T, Souvatzoglou M, Beer AJ, Ruffani A, Haller B, Graner FP, Kubler H, Haberhorn U, Eisenhut M, Wester HJ, Gschwend JE, Schwaiger M. Evaluation of hybrid (6)(8) Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J Nucl Med. 2015;56(5):668–674. doi: 10.2967/jnumed.115.154153. - DOI - PubMed
-
- Afshar-Oromieh A, Avtzi E, Giesel FL, Holland-Letz T, Linhart HG, Eder M, Eisenhut M, Boxler S, Hadaschik BA, Kratochwil C, Weichert W, Kopka K, Debus J, Haberkorn U. The diagnostic value of PET/CT imaging with the (68) Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2015;42(2):197–120. doi: 10.1007/s00259-014-2949-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
