

Comment
doi: 10.1183/13993003.04397-2020.
Print 2021 Aug.
Intrapulmonary bronchopulmonary anastomoses in COVID-19 respiratory failure
Affiliations
- PMID: 33863743
- PMCID: PMC8051184
- DOI: 10.1183/13993003.04397-2020
Item in Clipboard
Comment
Intrapulmonary bronchopulmonary anastomoses in COVID-19 respiratory failure
Eur Respir J.
.
Abstract
Open intrapulmonary bronchopulmonary anastomoses (IBA) were identified in COVID-19 patients who died of respiratory failure. IBA may be the microanatomical basis of intrapulmonary right to left shunt leading to severe hypoxaemia in COVID-19.
Conflict of interest statement
Conflict of interest: C. Galambos has nothing to disclose. Conflict of interest: D. Bush has nothing to disclose. Conflict of interest: S.H. Abman has nothing to disclose.
Figures
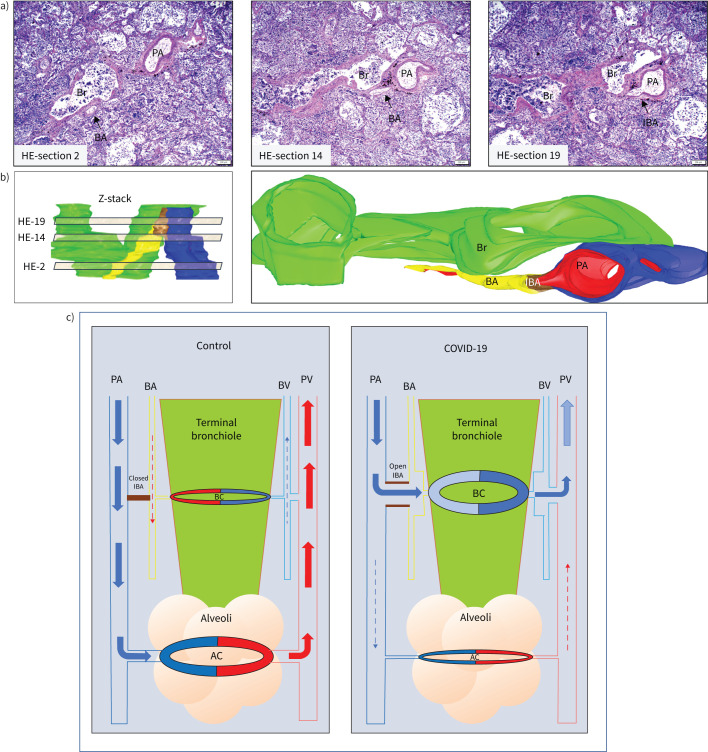
The combination of serial haematoxylin–eosin (HE) sections, and three-dimensional (3D) image reconstruction identifies recruited intrapulmonary bronchopulmonary anastomoses (IBA) in coronavirus disease 2019 (COVID-19) patients. a) Three representative images from the 30 serial HE sections analysed. Z-stack of HE sections showing an area of broncho-arterial bundle was first created (panel b, left: virtual light brown sections represent the approximate areas of the numbered HE sections in the Z stack) and a 3D image with oblique representation was reconstructed (panel b, right). There is a wide open IBA (brown in 3D image, small arrow in HE section 19) that connects the pulmonary artery (PA, blue) with the bronchial artery (BA, yellow). The bronchiole (Br) is green and endothelium of BA, IBA and PA is highlighted by red colour. Scale bars: 200 μm. c) Schematic demonstrating the microanatomy of intrapulmonary right-to-left shunt. Pulmonary blood flow in the distal lung at the terminal bronchiolar level is rearranged in COVID-19 patients. In the normal lung (left panel), the deoxygenated blood (blue arrow) in the pulmonary arteries (PA) enters the alveolar capillary bed (AC) for gas exchange, and the oxygenated blood (red arrows) is collected via pulmonary veins (PV) and enters the left heart. A small amount of oxygenated blood (red dashed arrow) supplies the terminal bronchiole (green colour) via the bronchial artery (BA) and the bronchiolar capillary network (BC). The deoxygenated blood (dashed blue arrow) is collected by the bronchial vein (BV) and consequently the pulmonary vein that enters the left heart. The IBAs (brown colour) are closed and no blood flow between pulmonary and bronchial vascular trees is present. In the COVID-19 lung (right panel), the majority of deoxygenated blood in the distal pulmonary arteries does not reach the alveolar capillary network for gas exchange (dashed blue arrow), but is redirected (blue arrows) through open IBAs towards the bronchial arteries and bronchial microcirculation, bypassing the alveolar capillary bed. The bronchial arteries, capillaries and veins are passively dilated due to the massive amount of blood coming from the right heart. The blood remains deoxygenated and is collected by the bronchial veins and enters the left heart via pulmonary veins, contributing to the profound systemic hypoxaemia experienced by COVID-19 patients.
Comment on
-
COVID-19 Does Not Lead to a "Typical" Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2020 May 15;201(10):1299-1300. doi: 10.1164/rccm.202003-0817LE. Am J Respir Crit Care Med. 2020. PMID: 32228035 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous