

The coexistence of asthma and COPD: risk factors, clinical history and lung function trajectories
- PMID: 33863744
- PMCID: PMC8613837
- DOI: 10.1183/13993003.04656-2020
The coexistence of asthma and COPD: risk factors, clinical history and lung function trajectories
Abstract
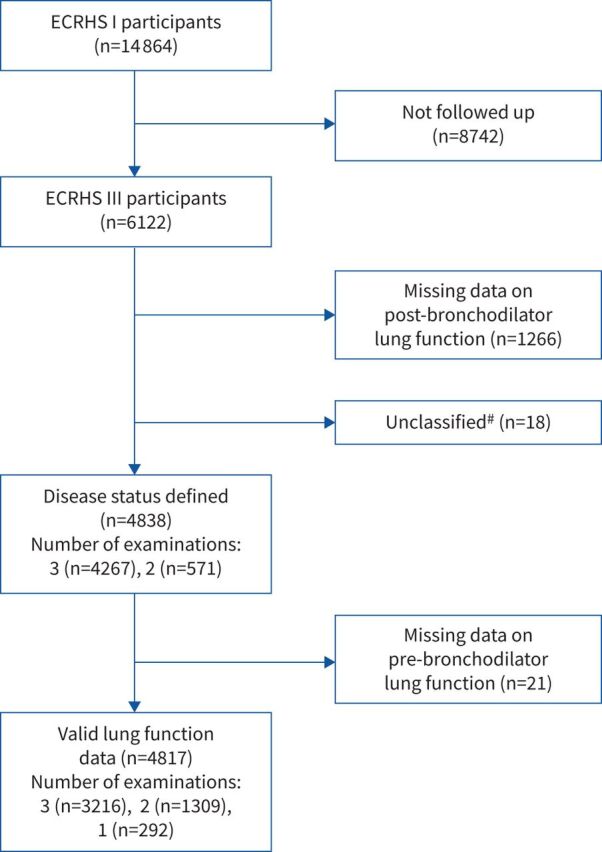
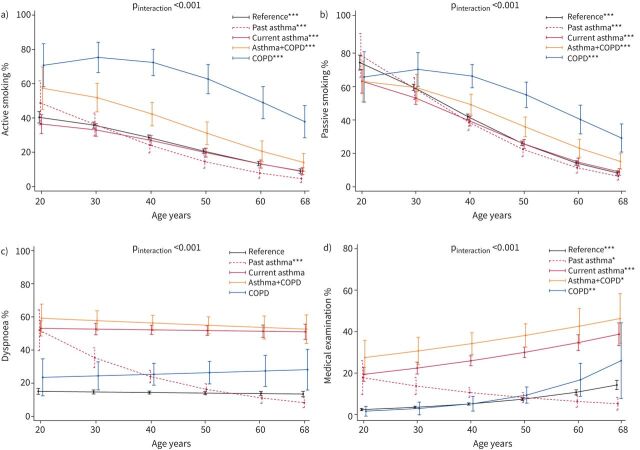
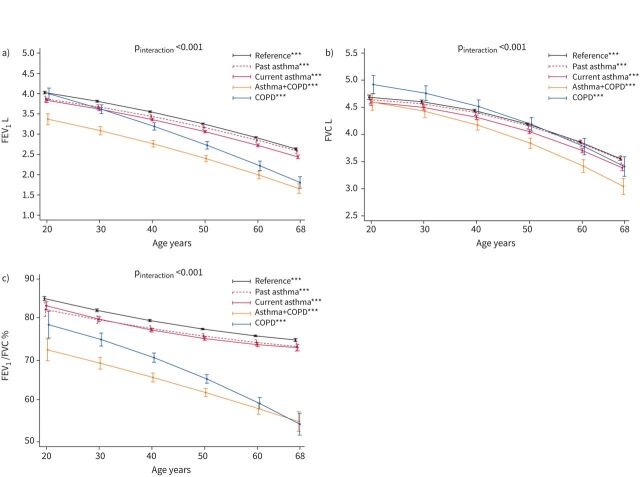
Patients with concomitant features of asthma and chronic obstructive pulmonary disease (COPD) have a heavy disease burden.Using data collected prospectively in the European Community Respiratory Health Survey, we compared the risk factors, clinical history and lung function trajectories from early adulthood to late sixties of middle-aged subjects with asthma+COPD (n=179), past (n=263) or current (n=808) asthma alone, COPD alone (n=111) or none of these (n=3477).Interview data and pre-bronchodilator forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) were obtained during three clinical examinations in 1991-1993, 1999-2002 and 2010-2013. Disease status was classified in 2010-2013, when the subjects were aged 40-68 years, according to the presence of fixed airflow obstruction (post-bronchodilator FEV1/FVC below the lower limit of normal), a lifetime history of asthma and cumulative exposure to tobacco or occupational inhalants. Previous lung function trajectories, clinical characteristics and risk factors of these phenotypes were estimated.Subjects with asthma+COPD reported maternal smoking (28.2%) and respiratory infections in childhood (19.1%) more frequently than subjects with COPD alone (20.9% and 14.0%, respectively). Subjects with asthma+COPD had an impairment of lung function at age 20 years that tracked over adulthood, and more than half of them had asthma onset in childhood. Subjects with COPD alone had the highest lifelong exposure to tobacco smoking and occupational inhalants, and they showed accelerated lung function decline during adult life.The coexistence between asthma and COPD seems to have its origins earlier in life compared to COPD alone. These findings suggest that prevention of this severe condition, which is typical at older ages, should start in childhood.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: A. Marcon has nothing to disclose. Conflict of interest: F. Locatelli has nothing to disclose. Conflict of interest: S.C. Dharmage has nothing to disclose. Conflict of interest: C. Svanes has nothing to disclose. Conflict of interest: J. Heinrich has nothing to disclose. Conflict of interest: B. Leynaert has nothing to disclose. Conflict of interest: P. Burney has nothing to disclose. Conflict of interest: A. Corsico has nothing to disclose. Conflict of interest: G. Caliskan has nothing to disclose. Conflict of interest: L. Calciano has nothing to disclose. Conflict of interest: T. Gislason has nothing to disclose. Conflict of interest: C. Janson has nothing to disclose. Conflict of interest: D. Jarvis has nothing to disclose. Conflict of interest: R. Jõgi received grants from the Estonian Research Council (Personal Research Grant n. 562), and personal fees for consultancy and lecturing from GSK, Boehringer and Novartis, and for travels/accommodation/meetings from GSK and Boehringer. Conflict of interest: T. Lytras has nothing to disclose. Conflict of interest: A. Malinovschi has nothing to disclose. Conflict of interest: N. Probst-Hensch has nothing to disclose. Conflict of interest: K. Toren has nothing to disclose. Conflict of interest: L. Casas has nothing to disclose. Conflict of interest: G. Verlato has nothing to disclose. Conflict of interest: J. Garcia-Aymerich has nothing to disclose. Conflict of interest: S. Accordini has nothing to disclose.
Figures
Comment in
-
Asthma, COPD and their overlap: coexistence or something more?Eur Respir J. 2021 Nov 25;58(5):2101329. doi: 10.1183/13993003.01329-2021. Print 2021 Nov. Eur Respir J. 2021. PMID: 34824127 No abstract available.
-
The coexistence of asthma and COPD: some considerations about prevalence and lung function decline.Eur Respir J. 2022 Mar 17;59(3):2200096. doi: 10.1183/13993003.00096-2022. Print 2022 Mar. Eur Respir J. 2022. PMID: 35115342 No abstract available.
References
-
- Global Initiative for Asthma . Global Strategy for Asthma Management and Prevention. 2020. www.ginasthma.org Date last accessed: July 22, 2020.
-
- Global Initiative for Chronic Obstructive Lung Disease . Global Strategy for the Diagnosis, Management and Prevention of COPD. 2020. https://goldcopd.org/ Date last accessed: July 29, 2020.
-
- American Thoracic Society . Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152: S77–S121. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous