

An integrated multi-omics analysis identifies prognostic molecular subtypes of non-muscle-invasive bladder cancer
- PMID: 33863885
- PMCID: PMC8052448
- DOI: 10.1038/s41467-021-22465-w
An integrated multi-omics analysis identifies prognostic molecular subtypes of non-muscle-invasive bladder cancer
Abstract
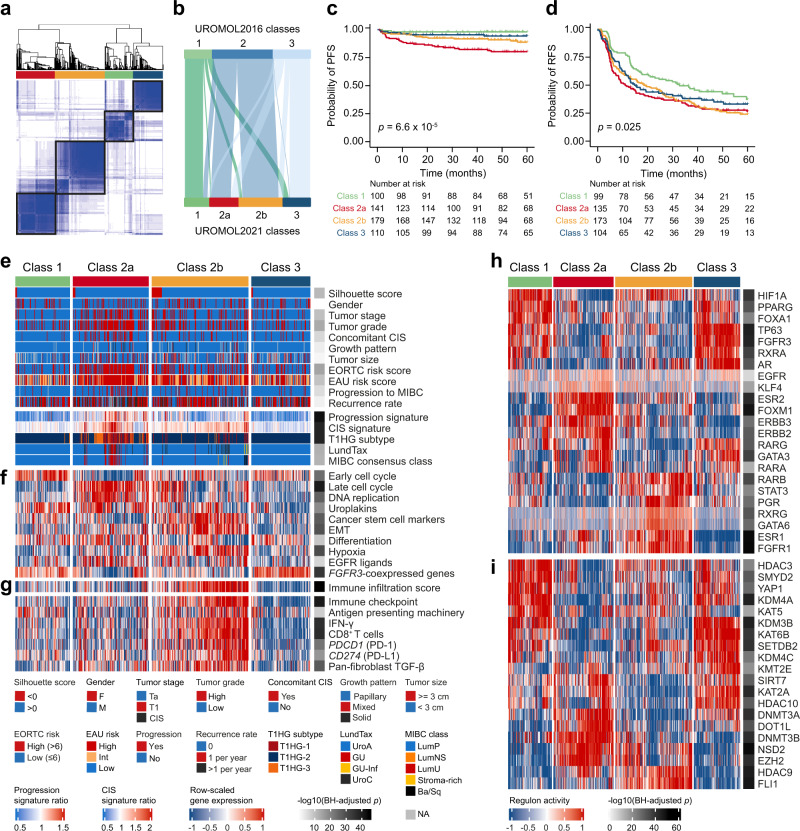
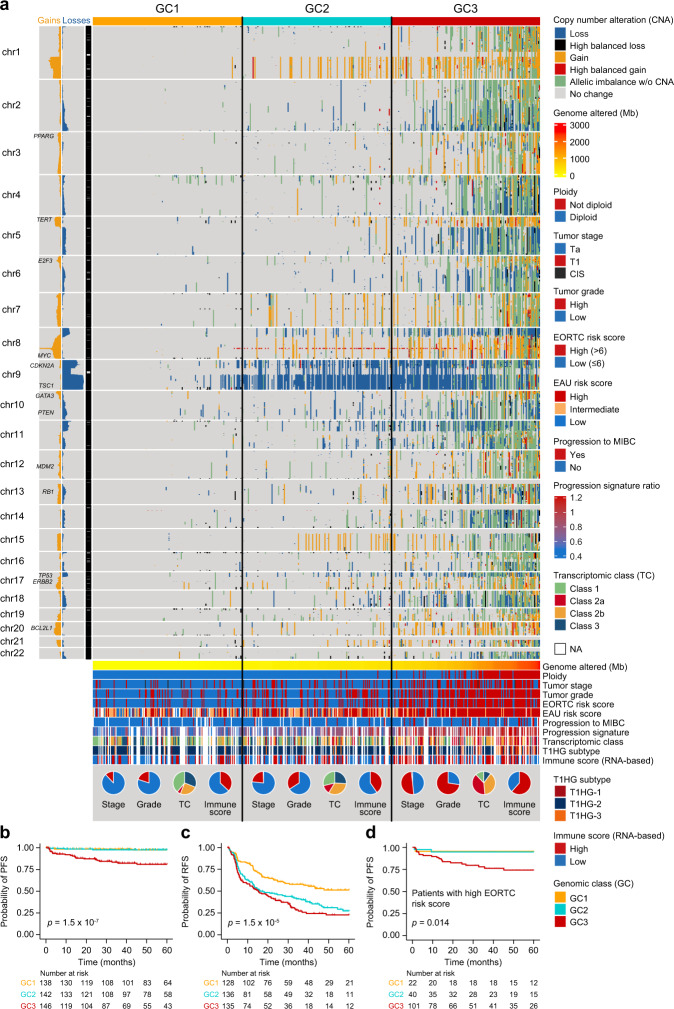
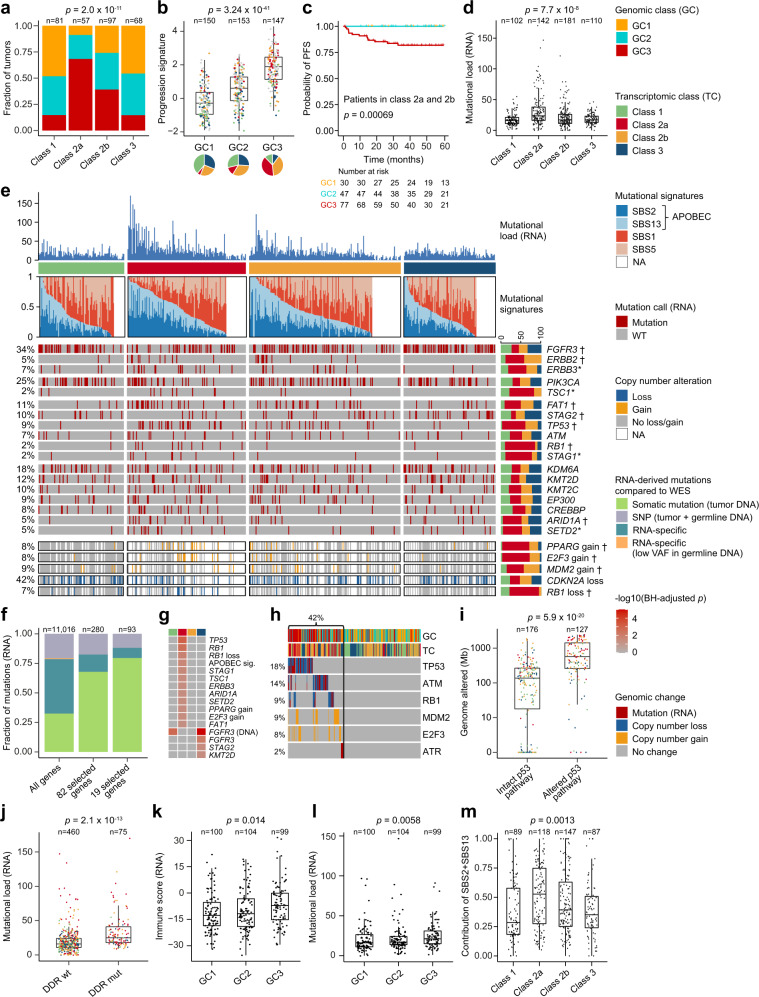
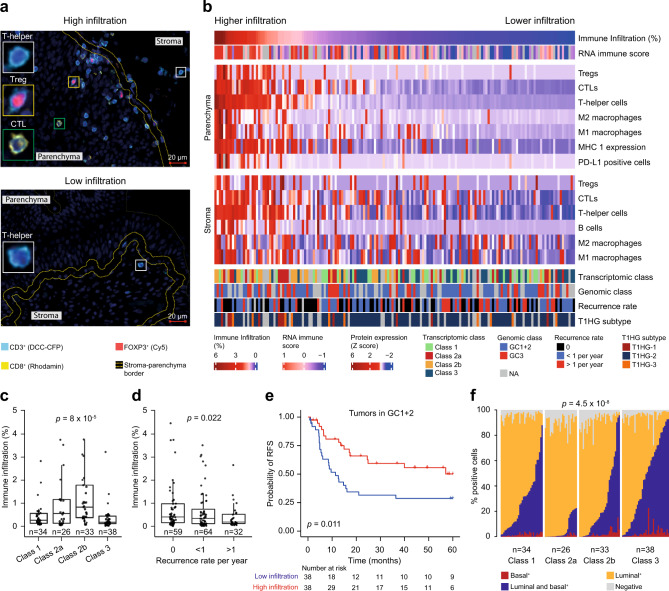
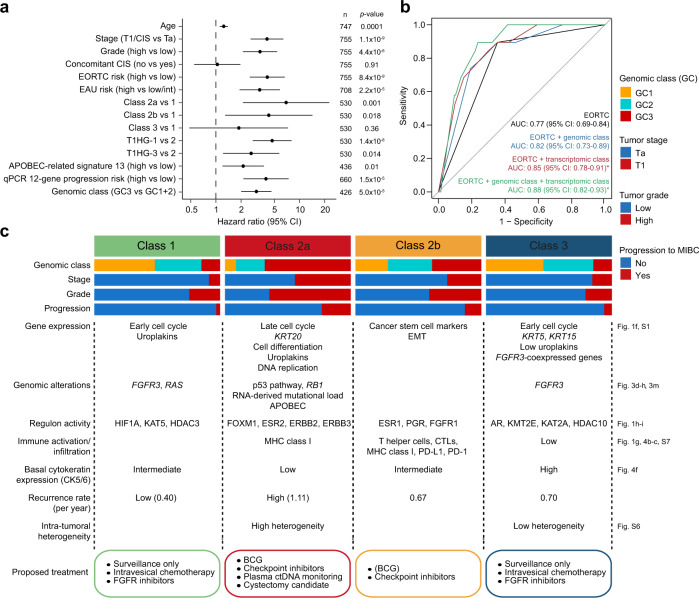
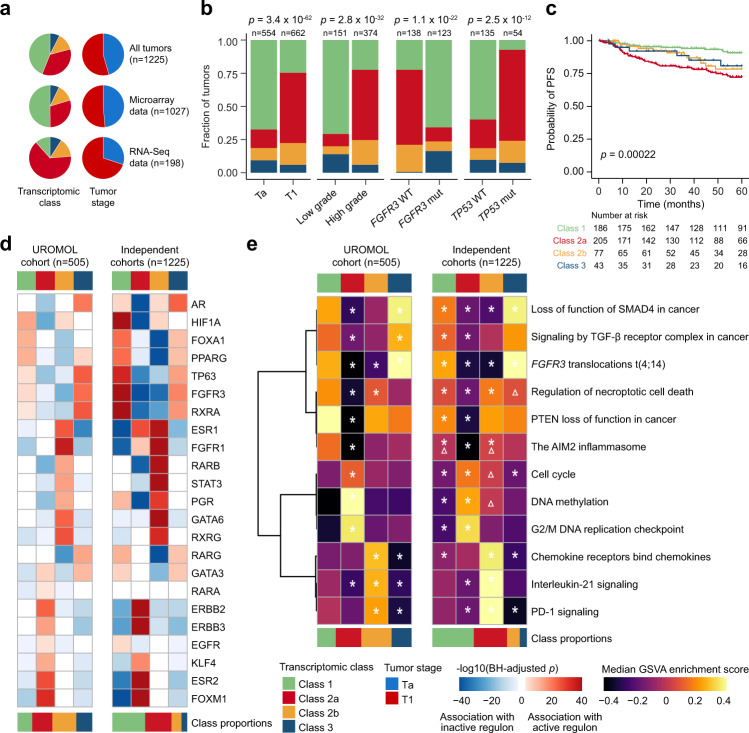
The molecular landscape in non-muscle-invasive bladder cancer (NMIBC) is characterized by large biological heterogeneity with variable clinical outcomes. Here, we perform an integrative multi-omics analysis of patients diagnosed with NMIBC (n = 834). Transcriptomic analysis identifies four classes (1, 2a, 2b and 3) reflecting tumor biology and disease aggressiveness. Both transcriptome-based subtyping and the level of chromosomal instability provide independent prognostic value beyond established prognostic clinicopathological parameters. High chromosomal instability, p53-pathway disruption and APOBEC-related mutations are significantly associated with transcriptomic class 2a and poor outcome. RNA-derived immune cell infiltration is associated with chromosomally unstable tumors and enriched in class 2b. Spatial proteomics analysis confirms the higher infiltration of class 2b tumors and demonstrates an association between higher immune cell infiltration and lower recurrence rates. Finally, the independent prognostic value of the transcriptomic classes is documented in 1228 validation samples using a single sample classification tool. The classifier provides a framework for biomarker discovery and for optimizing treatment and surveillance in next-generation clinical trials.
Conflict of interest statement
L.D. has sponsored research agreements with C2i-genomics, Natera, AstraZeneca and Ferring, and has an advisory/consulting role at Ferring. J.B.J. has sponsored research agreements with Medac, Photocure ASA, Cephaid, Nucleix, Astellas and Ferring, and has an advisory board role at Olympus Europe, Cephaid and Ferring. J.D.R. is involved in a sponsored scientific study or trial with Pacific Edge Biotechnologies, MDxHealth and Urogen Pharma, is a consultant for Urogen Pharma, and has an investment interest in American Kidney Stone Management. J.J.M. is a consultant for Ferring, AstraZeneca, Janssen and participated in advisory boards for Foundation Medicine and Nucleix. R.T.B. has contributed to advisory boards for Olympus Medical Systems & Janssen, and undertakes research funded by UroGen Pharma and QED Therapeutics. The following authors declare no competing interests: S.V.L., F.P., P.L., A.T., C.S.G., K.B.D., T.S., I.N., E.C., M.S., N.J.B., L.M., G.G.H., A.C.P., V.W., M.O.G., M.H., G.S., M.H., T.S., K.M., A.R., R.M., B.J., X.L., D.D., D.G.W., A.G., C.D.H., J.I.W., U.S., D.S., K.E.M.K., T.M., D.J.D., M.A.K., T.S., A.H., E.C.Z., P.U.M., N.M., and F.X.R.
Figures
Comment in
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2022 Mar;207(3):733-734. doi: 10.1097/JU.0000000000002358. Epub 2021 Dec 15. J Urol. 2022. PMID: 34905949 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
