

A computed tomography cadaveric study of the radiological anatomy of the patella: the size of the patella correlates with bone bridge between tunnels and R angles are introduced for safe tunnel drilling during MPFL reconstruction
- PMID: 33864169
- PMCID: PMC8052390
- DOI: 10.1186/s40634-021-00348-9
A computed tomography cadaveric study of the radiological anatomy of the patella: the size of the patella correlates with bone bridge between tunnels and R angles are introduced for safe tunnel drilling during MPFL reconstruction
Abstract
Purpose: To measure the safe range of angles during tunnel drilling and map ideal patella tunnel placement with the use of preoperative computed tomography (CT) scan and compare results after medial patellofemoral ligament (MPFL) reconstruction using a hardware-free patellar fixation technique with two semi-patellar tunnels between a) a free-hand technique, and b) its modification with the use of an anterior cruciate ligament (ACL) tibia aiming device.
Methods: CT scan was performed on 30 fresh-frozen cadaveric knees a) prior to any intervention and b) after MPFL reconstruction. For MPFL reconstruction, specimens were randomly allocated to 1) Group A, which consisted of knees operated with free-hand, hardware-free patellar fixation technique with two semi-patellar tunnels and 2) Group B, which consisted of knees operated on with a technique modification with the ACL tibia device.
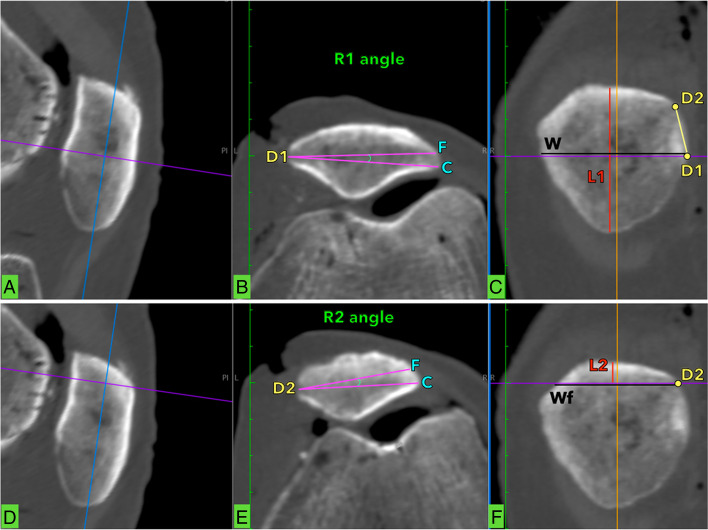
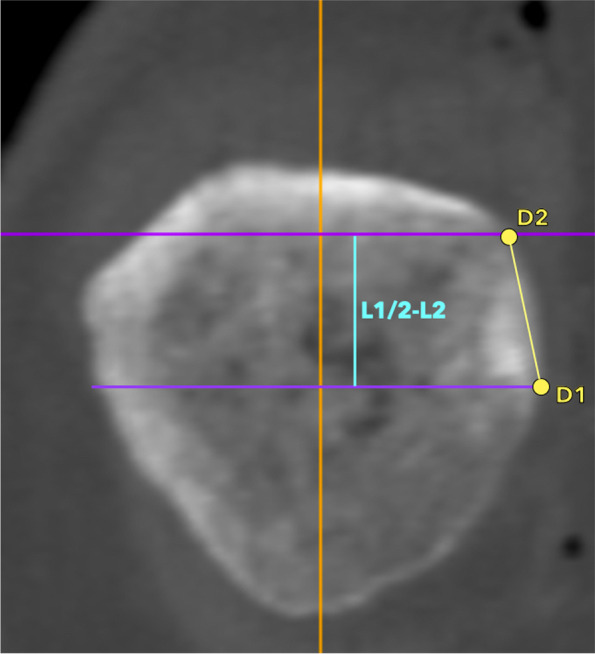
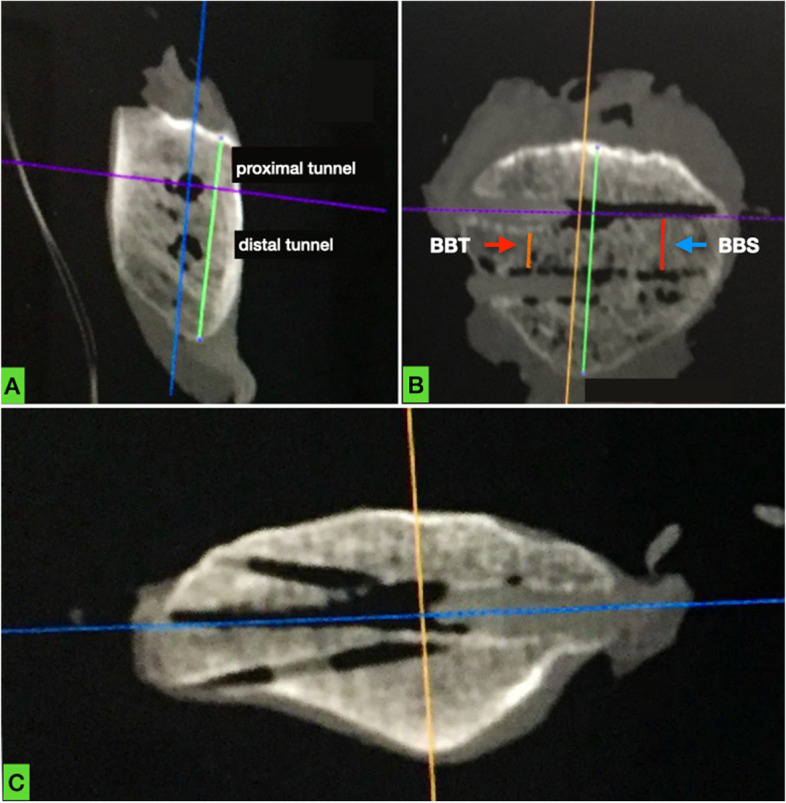
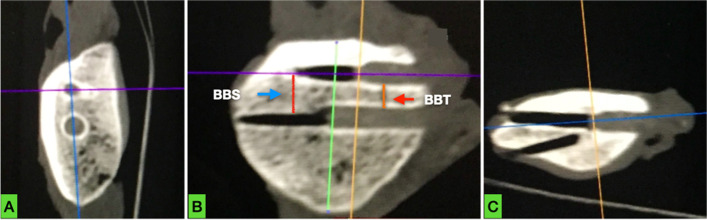
Patellar measurements: L1 was the maximal patellar length. L2 was the minimum possible distance of placement for the upper tunnel from the proximal pole of the patella. The maximum bone bridge between tunnels was calculated as half of L1 minus the L2 distance (L1/2-L2). We also measured R1 and R2 angles at the proximal and distal tunnel that represent safe angles at the entry point during tunnel drilling (without breaching the anterior cortex or articular cartilage).
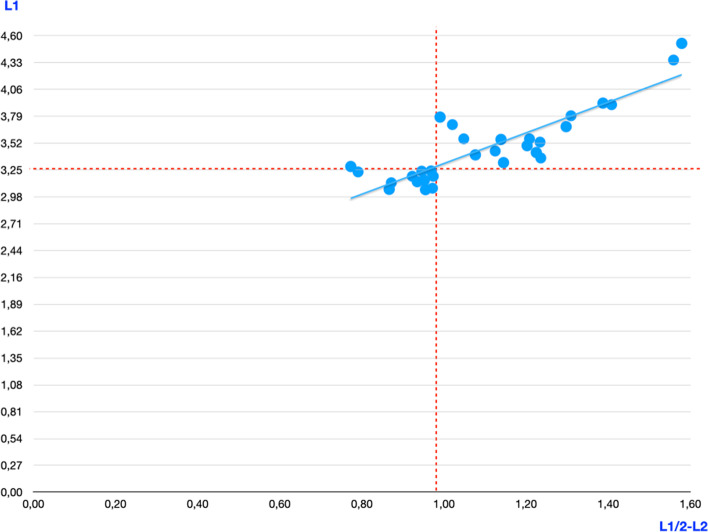
Results: Preoperatively, mean L1 was 3.45 cm (range 3.05-4.52). Mean L2 was 0.62 cm (range 0.49-0.89). The mean maximum possible bone bridge between tunnels (L1/2-L2) was 1.1 cm (range 0.77-1.58). R1 was 6.050 (range 4.78-7.44), R2 was 6.640 (range 4.57-9.03), and their difference reached statistical significance (p = 0.03). Postoperatively, in group A, in 4 out of 15 patellas, multiple attempts were made during tunnel drilling in order to avoid anterior cortex or cartilage breaching. In group B, all tunnels were correctly drilled with the first attempt. Bone bridge between tunnels was significantly shorter postoperatively (0.93 cm, p < 0.01).
Conclusion: Small-size patellae correlate with short maximum bone bridge between tunnels, which makes anatomic, double-bundle, hardware-free patella fixation, with two semi-patellar tunnels MPFL reconstruction challenging. Furthermore, R angles create a narrow window to avoid intraoperative breaching, rendering the use of the ACL tibia device an extremely useful instrument.
Level of evidence: II.
Keywords: Cadaveric; Computed tomography; Double-bundle MPFL; Patella instability; Patella tunnels; Radiological anatomy.
Conflict of interest statement
None.
Figures
Similar articles
-
Reconstruction of the medial patellofemoral ligament using two blind transverse semi-patella tunnels and an implant-free technique for patellar fixation: a technical note.J Orthop Surg Res. 2021 Jan 7;16(1):25. doi: 10.1186/s13018-020-02161-z. J Orthop Surg Res. 2021. PMID: 33413498 Free PMC article.
-
The effect of femoral tunnel position and graft tension on patellar contact mechanics and kinematics after medial patellofemoral ligament reconstruction.Am J Sports Med. 2014 Feb;42(2):364-72. doi: 10.1177/0363546513509230. Epub 2013 Nov 25. Am J Sports Med. 2014. PMID: 24275861
-
Transpatellar bone tunnels perforating the lateral or anterior cortex increase the risk of patellar fracture in MPFL reconstruction: a finite element analysis and survey of the International Patellofemoral Study Group.Knee Surg Sports Traumatol Arthrosc. 2022 May;30(5):1620-1628. doi: 10.1007/s00167-021-06682-w. Epub 2021 Jul 31. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 34333671
-
Tunnel widening in single- versus double-bundle anterior cruciate ligament reconstructed knees.Knee Surg Sports Traumatol Arthrosc. 2017 Apr;25(4):1316-1327. doi: 10.1007/s00167-016-4204-0. Epub 2016 Jun 21. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27329174 Free PMC article. Review.
-
Anatomic Double-Bundle Medial Patellofemoral Ligament Reconstruction with Autologous Semitendinosus: Aperture Fixation Both at the Femur and the Patella.Joints. 2017 Oct 4;5(4):256-260. doi: 10.1055/s-0037-1607192. eCollection 2017 Dec. Joints. 2017. PMID: 29270566 Free PMC article. Review.
Cited by
-
The 100 Top-Cited Articles on Medial Patellofemoral Ligament: A Bibliometric Analysis and Review.Orthop J Sports Med. 2024 Jan 31;12(1):23259671231223525. doi: 10.1177/23259671231223525. eCollection 2024 Jan. Orthop J Sports Med. 2024. PMID: 38304053 Free PMC article.
References
-
- Fleiss J (1986) The design and analysis of clinical experiments. Wiley
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
