

Effects of Gocovri (Amantadine) Extended Release Capsules on Non-Motor Symptoms in Patients with Parkinson's Disease and Dyskinesia
- PMID: 33864229
- PMCID: PMC8140024
- DOI: 10.1007/s40120-021-00246-3
Effects of Gocovri (Amantadine) Extended Release Capsules on Non-Motor Symptoms in Patients with Parkinson's Disease and Dyskinesia
Abstract
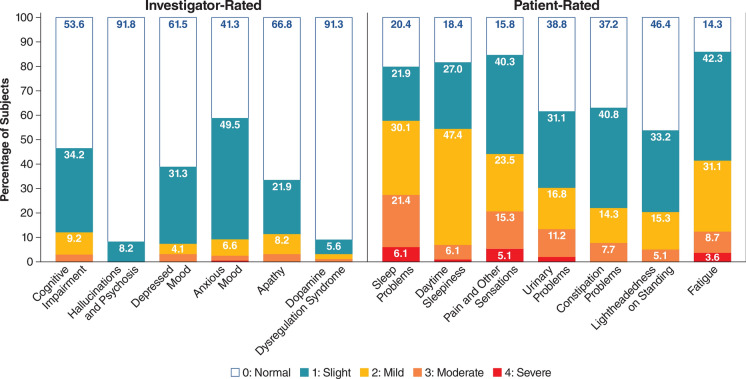
Introduction: Gocovri (amantadine) extended release capsules are approved for treatment of dyskinesia and as a levodopa adjunct for OFF episodes in patients with Parkinson's disease (PD). We report treatment-related effects on non-motor symptoms (NMS) assessed as secondary outcomes in two trials using the Movement Disorder Society-Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Part I.
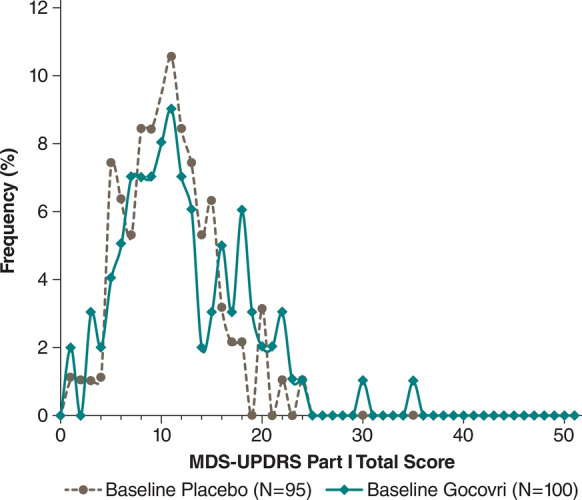
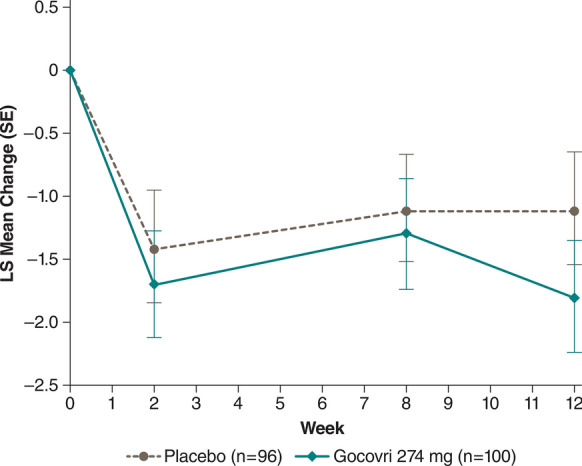
Methods: EASE LID and EASE LID 3 enrolled levodopa-treated patients with PD and ≥ 1 h/day ON time with troublesome dyskinesia. Patients were randomized to Gocovri (274 mg) or placebo taken daily at bedtime. Treatment differences from baseline to week 12 in MDS-UPDRS Part I were evaluated for the pooled population (N = 196) from both trials. Correlation analyses of NMS (MDS-UPDRS Part I) with dyskinesia using Unified Dyskinesia Rating Scale (UDysRS) scores were performed.
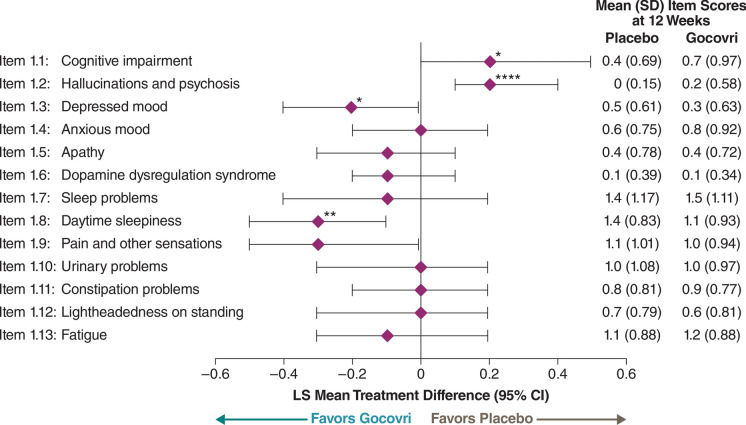
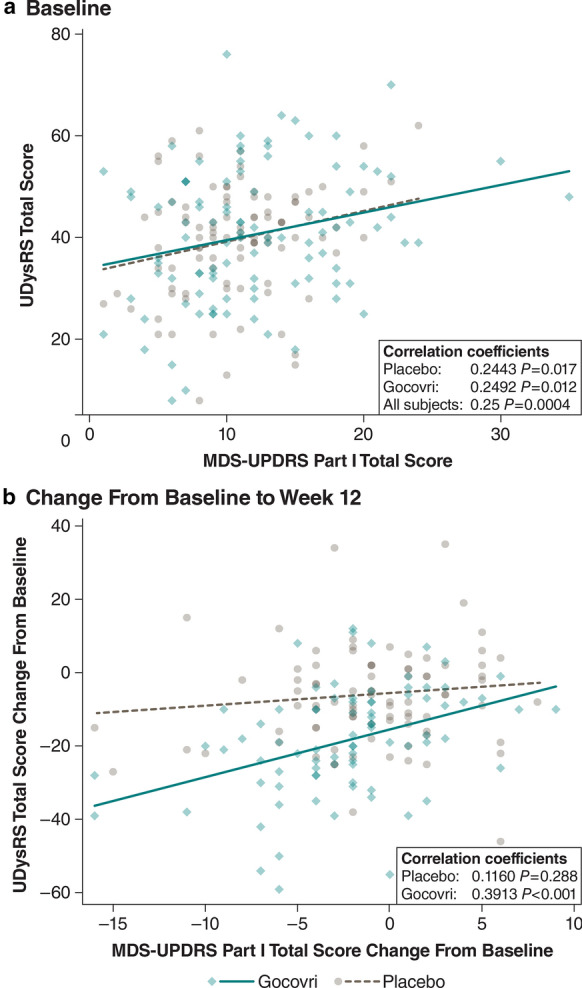
Results: For changes in the MDS-UPDRS Part I items, the treatment difference favored Gocovri in daytime sleepiness (P = 0.006) and depression (P = 0.049) scores, but favored placebo in cognitive impairment (P = 0.038), and hallucinations and psychosis (P < 0.001) scores. The treatment difference for the changes in total Part I score was -0.8, favoring Gocovri (P = 0.22). At baseline, MDS-UPDRS Part I modestly correlated with UDysRS score (r +0.25, P < 0.001), and improvement in NMS correlated with improvement in dyskinesia at week 12 for Gocovri (r +0.39, P < 0.001) but not placebo (r +0.12, P = 0.29). The most commonly reported adverse events for Gocovri were hallucination (21%); dizziness, dry mouth, and peripheral edema (16% each); and constipation, falls, and orthostatic hypotension (13% each).
Conclusion: This post hoc analysis shows potential benefit with Gocovri treatment for the NMS of daytime sleepiness and depression in dyskinetic PD patients. Overall, improvement in NMS scores correlated with improvement in dyskinesia.
Trial registration: ClinicalTrials.gov identifiers: NCT02136914 and NCT02274766.
Keywords: Amantadine; Depression; Depressive disorder; Dyskinesias; Hallucinations; Parkinson’s disease; Sleep.
Figures
References
-
- Chaudhuri KR, Martinez-Martin P, Schapira AH, Stocchi F, Sethi K, Odin P, et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson's disease: the NMSQuest study. Mov Disord. 2006;21(7):916–923. doi: 10.1002/mds.20844. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
