

Global estimates of expected and preventable cervical cancers among girls born between 2005 and 2014: a birth cohort analysis
- PMID: 33864738
- PMCID: PMC8225515
- DOI: 10.1016/S2468-2667(21)00046-3
Global estimates of expected and preventable cervical cancers among girls born between 2005 and 2014: a birth cohort analysis
Abstract
Background: WHO has launched an initiative aiming to eliminate cervical cancer as a public health problem. Elimination is a long-term target that needs long-lasting commitment. To support local authorities in implementing human papillomavirus (HPV) vaccination, we provide regional and country-specific estimates of cervical cancer burden and the projected impact of HPV vaccination among today's young girls who could develop cervical cancer if not vaccinated.
Methods: The expected number of cervical cancer cases in the absence of vaccination among girls born between 2005 and 2014 was quantified by combining age-specific incidence rates from GLOBOCAN 2018 and cohort-specific mortality rates by age from UN demographic projections. Preventable cancers were estimated on the basis of HPV prevalence reduction attributable to vaccination and the relative contribution of each HPV type to cervical cancer incidence. We assessed the number of cervical cancer cases preventable through vaccines targeting HPV types 16 and 18, with and without cross-protection, and through vaccines targeting HPV types 16, 18, 31, 33, 45, 52, and 58.
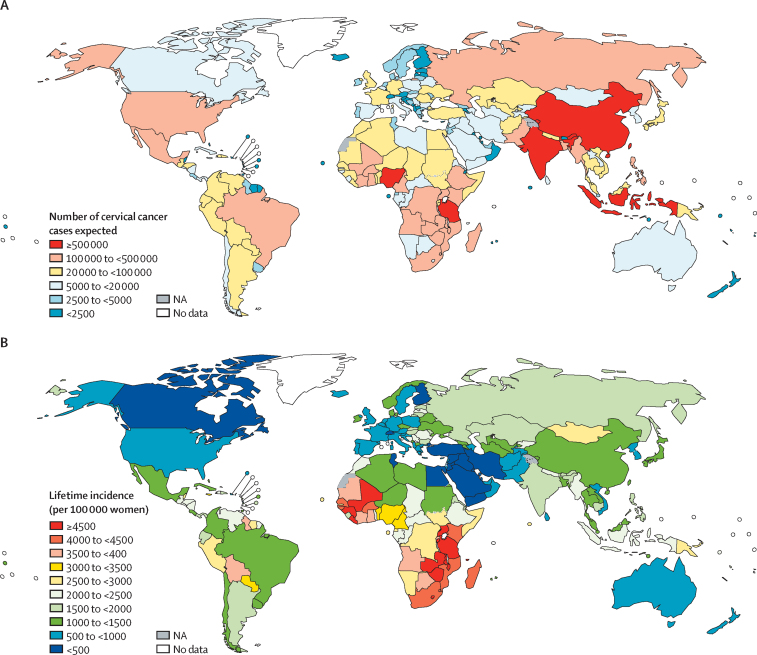
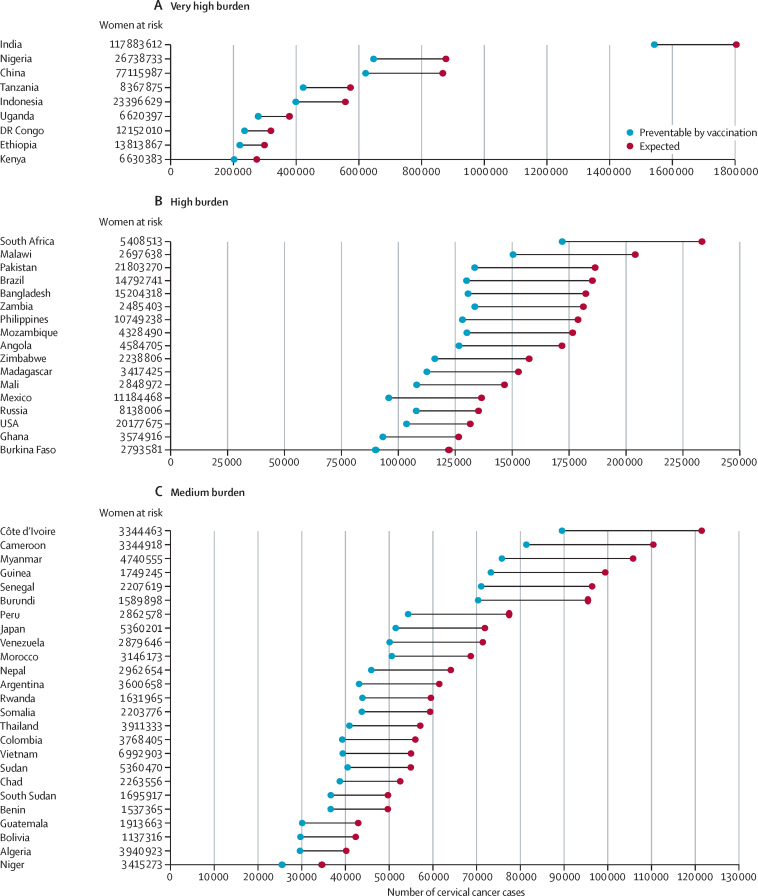
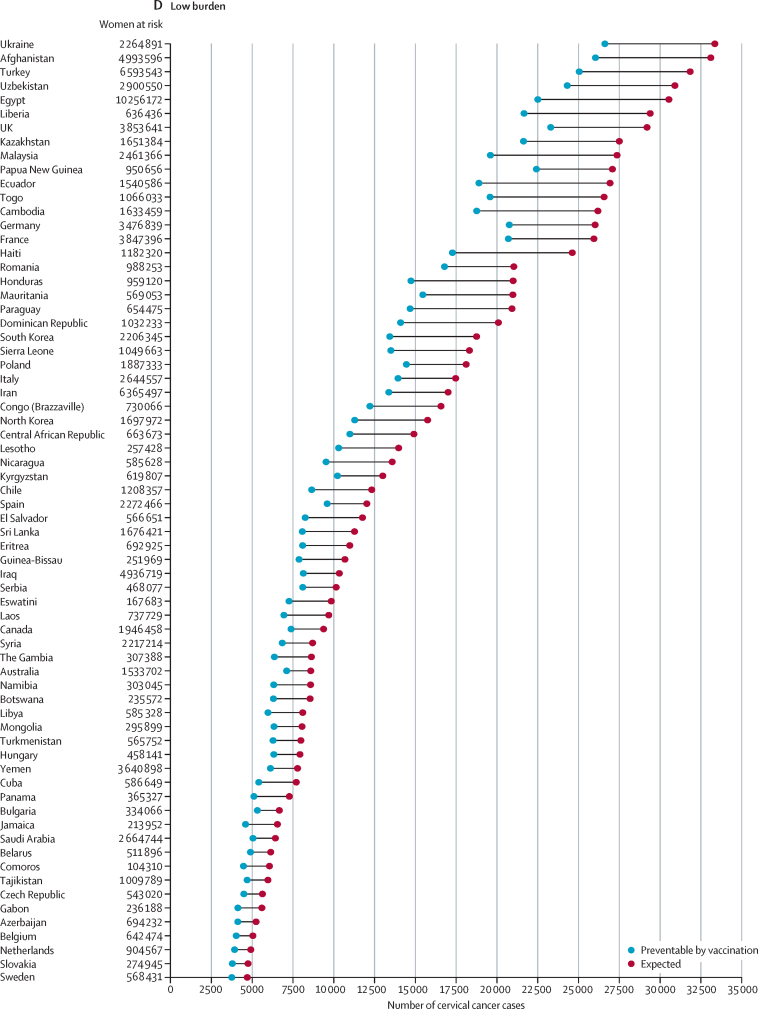
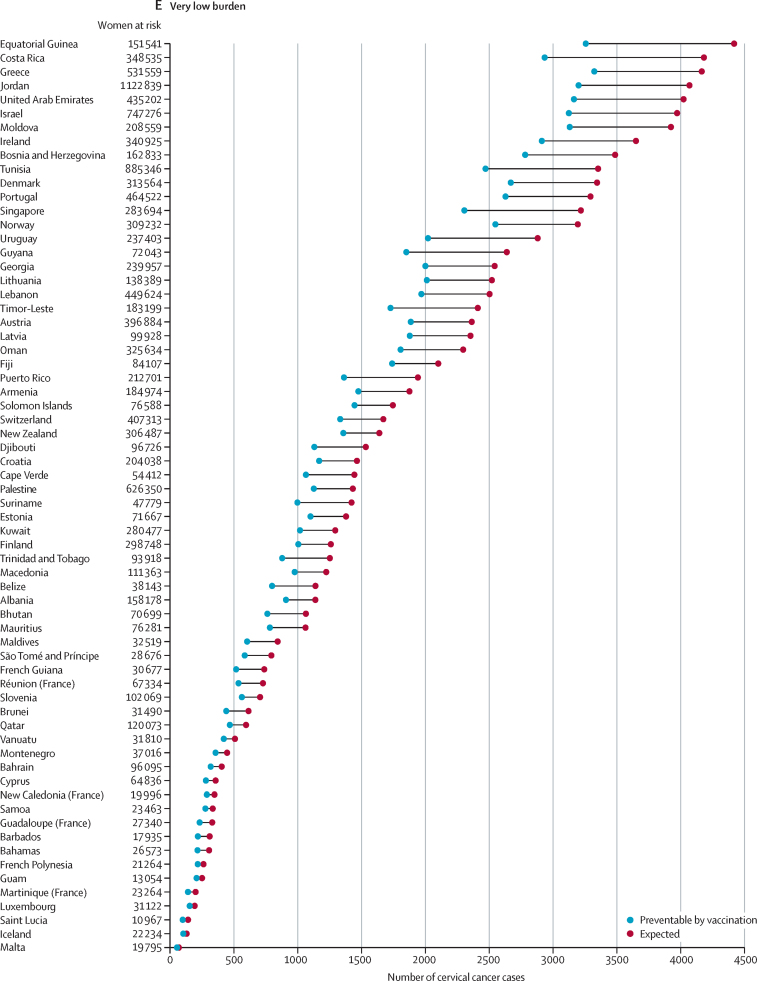
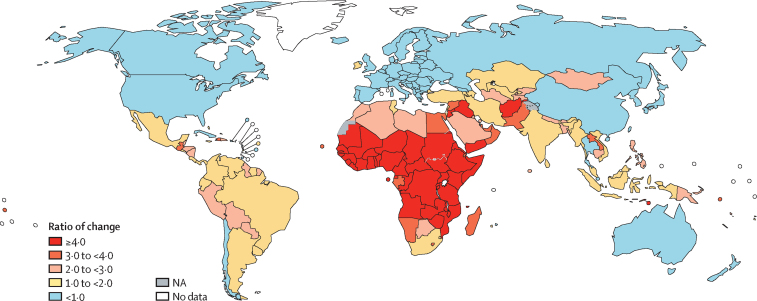
Findings: Globally, without vaccination, the burden of cervical cancer in these birth cohorts is expected to reach 11·6 million (95% uncertainty interval 11·4-12·0) cases by 2094. Approximately 75% of the burden will be concentrated in 25 countries mostly located in Africa and Asia, where the future number of cases is expected to increase manyfold, reaching 5·6 million (5·4-6·0) cases in Africa and 4·5 million (4·4-4·6) cases in Asia. Worldwide immunisation with an HPV vaccine targeted to HPV types 16 and 18, with cross-protection against HPV types 31, 33, and 45, could prevent about 8·7 million (8·5-9·0) cases.
Interpretation: Detailed estimates of the increasing burden of cervical cancer and projected impact of HPV vaccination is of immediate relevance to public health decision makers. Shifting the focus of projections towards recently born girls who could develop cervical cancer if not vaccinated is fundamental to overcome stakeholders' hesitancy towards HPV vaccination.
Funding: Bill & Melinda Gates Foundation, Canadian Institutes of Health Research.
Copyright © 2021 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests ELF has received grants to his university and personal fees from Merck, outside of the submitted work. ELF has a patent “Methylation markers in cervical cancer” pending to his university. The other authors declare no competing interests.
Figures

Similar articles
-
Evidence-based impact projections of single-dose human papillomavirus vaccination in India: a modelling study.Lancet Oncol. 2022 Nov;23(11):1419-1429. doi: 10.1016/S1470-2045(22)00543-5. Epub 2022 Sep 26. Lancet Oncol. 2022. PMID: 36174583 Free PMC article.
-
Effects of updated demography, disability weights, and cervical cancer burden on estimates of human papillomavirus vaccination impact at the global, regional, and national levels: a PRIME modelling study.Lancet Glob Health. 2020 Apr;8(4):e536-e544. doi: 10.1016/S2214-109X(20)30022-X. Epub 2020 Feb 24. Lancet Glob Health. 2020. PMID: 32105613 Free PMC article.
-
Estimation of the potential overall impact of human papillomavirus vaccination on cervical cancer cases and deaths.Vaccine. 2014 Feb 3;32(6):733-9. doi: 10.1016/j.vaccine.2013.11.049. Epub 2013 Nov 26. Vaccine. 2014. PMID: 24291200
-
Human papillomavirus vaccines: current status and future prospects.Drugs. 2010 Jun 18;70(9):1079-98. doi: 10.2165/10898580-000000000-00000. Drugs. 2010. PMID: 20518577 Review.
-
The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonavalent vaccine prevent?Euro Surveill. 2018 Oct;23(41):1700737. doi: 10.2807/1560-7917.ES.2018.23.41.1700737. Euro Surveill. 2018. PMID: 30326995 Free PMC article. Review.
Cited by
-
Serum IL-6 Level Predicts the Prognosis and Diagnosis in Cervical Cancer Patients.Int J Womens Health. 2022 May 3;14:655-663. doi: 10.2147/IJWH.S347740. eCollection 2022. Int J Womens Health. 2022. PMID: 35547839 Free PMC article.
-
Approximating missing epidemiological data for cervical cancer through Footprinting: A case study in India.Elife. 2023 May 25;12:e81752. doi: 10.7554/eLife.81752. Elife. 2023. PMID: 37227260 Free PMC article.
-
Towards elimination of cervical cancer - human papillomavirus (HPV) vaccination and cervical cancer screening in Asian National Cancer Centers Alliance (ANCCA) member countries.Lancet Reg Health West Pac. 2023 Aug 1;39:100860. doi: 10.1016/j.lanwpc.2023.100860. eCollection 2023 Oct. Lancet Reg Health West Pac. 2023. PMID: 37576906 Free PMC article. Review.
-
Women's Participation in Pap Smear Screening in a Developing Country: Evidence for Improving Health Systems.Front Oncol. 2021 Jun 15;11:642841. doi: 10.3389/fonc.2021.642841. eCollection 2021. Front Oncol. 2021. PMID: 34211837 Free PMC article.
-
Human papillomavirus vaccine effect against human papillomavirus infection in Rwanda: evidence from repeated cross-sectional cervical-cell-based surveys.Lancet Glob Health. 2023 Jul;11(7):e1096-e1104. doi: 10.1016/S2214-109X(23)00193-6. Epub 2023 May 16. Lancet Glob Health. 2023. PMID: 37207683 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
