

A novel NCOR2-NTRK1 fusion detected in a patient of lung adenocarcinoma and response to larotrectinib: a case report
- PMID: 33865348
- PMCID: PMC8052639
- DOI: 10.1186/s12890-021-01490-x
A novel NCOR2-NTRK1 fusion detected in a patient of lung adenocarcinoma and response to larotrectinib: a case report
Abstract
Background: The identification of NTRK fusions in tumours has become critically important due to the actionable events predictive of response to TRK inhibitor. It is not clear whether the NTRK breakpoint location is different for response to targeted therapy and NTRK fusions affects the efficacy of immunotherapy.
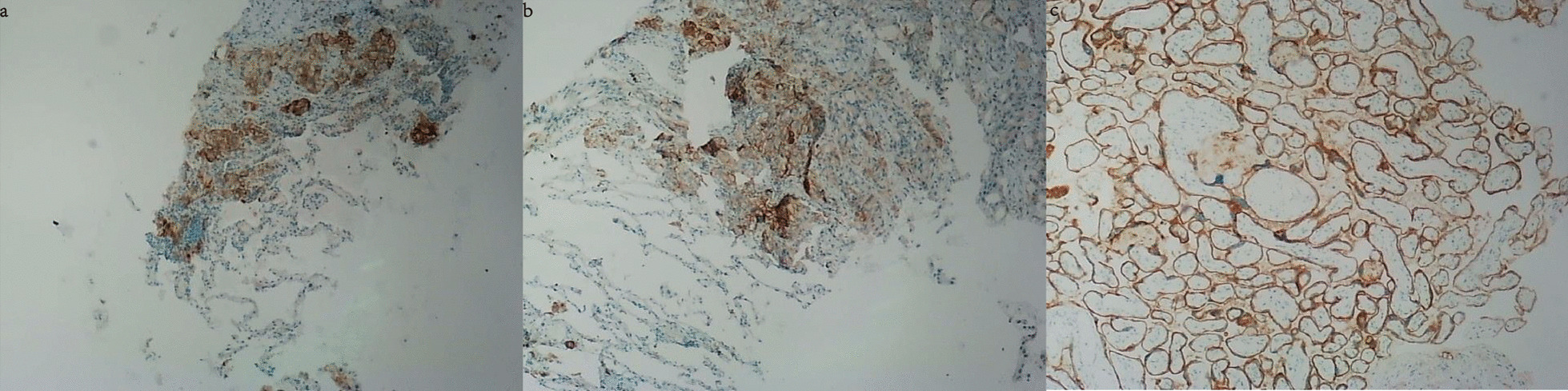
Case presentation: Here we reported a 60-year-old female diagnosed with advanced lung adenocarcinoma. NGS-based molecular profiling identified a novel NCOR2-NTRK1 fusion and high tumor mutational burden (TMB) (58.58 mutations/Mb) in this case. Additionally, program death-ligand 1 (PD-L1) expression was detected in 20-30% of the tumor cells by immunohistochemical (IHC) staining. The patient received treatment with anti-PD-1 immune checkpoint inhibitor of camrelizumab. After two cycles of treatment, the CT scan showed some tumor nodules were still enlarged, indicating disease progression. She was then changed to TRK inhibitor larotrectinib. One month later, the CT scan showed the volume of some lesions started to decrease, and no metastasis lesions were found. The patient then continued the administration of larotrectinib, and some lesion sizes were significantly reduced or even disappeared in the next few months. Currently, this patient is still alive.
Conclusions: Altogether, this report provided a new driver of lung adenocarcinoma expanded the mutational spectrum of NTRK1 fusion variants and suggested using larotrectinib as the targeted therapy is more effective than anti-PD-1 inhibitor in lung adenocarcinoma harboring with NTRK fusion, positive PD-L1 expression, and high TMB simultaneously.
Keywords: Case report; Larotrectinib; Lung adenocarcinoma; NTRK fusion; PD-L1.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form. The authors declare that they have no competing interests.
Figures


References
-
- Rizvi H, Sanchez-Vega F, La K, Chatila W, Jonsson P, Halpenny D, et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol. 2018;36(7):633–641. doi: 10.1200/JCO.2017.75.3384. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
